A Wide Spectrum of Axial Mesodermal Dysplasia Complex With Rhombencephalic Anomaly: A Case Report
- Affiliations
-
- 1Department of Physical Medicine and Rehabilitation, Chonbuk National University Medical School, Jeonju, Korea. shpark0130@chonbuk.ac.kr
- KMID: 2155179
- DOI: http://doi.org/10.5535/arm.2016.40.1.162
Abstract
- Axial mesodermal dysplasia complex (AMDC) arises in variable combinations of craniocaudal anomalies such as musculoskeletal deformities, neuroschisis, or rhombencephalic developmental disorders. To the best of our knowledge, the co-existence of AMDC with associated musculoskeletal anomalies, medullary neuroschisis with mirror movements, and cranial nerve anomalies has not yet been reported. Here, we report the case of a 4-year-old boy whose clinical features were suggestive of Goldenhar syndrome and Poland syndrome with Sprengel deformity. Moreover, he showed mirror movements in his hands suspected of rhombencephalic malformation, and infranuclear-type facial nerve palsy of the left side of his face, the opposite side to the facial anomalies of Goldenhar syndrome. After conducting radiological studies, he was diagnosed with medullary neuroschisis without pontine malformations and Klippel-Feil syndrome with rib anomalies. Based on these findings, we propose that clinical AMDC can be accompanied by a wide variety of musculoskeletal defects and variable degrees of central nervous system malformations. Therefore, in addition to detailed physical and neurological examinations, imaging studies should be considered in AMDC.
MeSH Terms
Figure
-
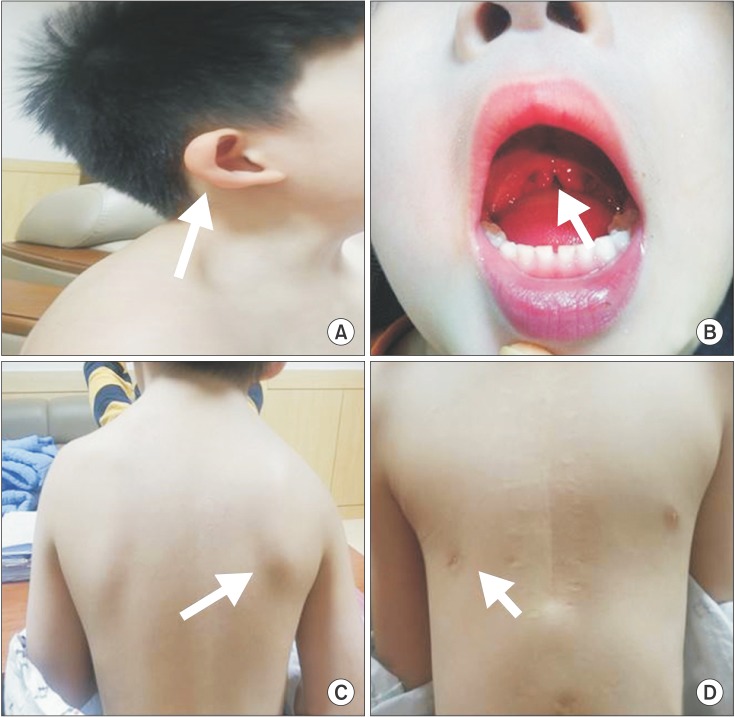
Fig. 1 Patient showing clinical features consisting of microtia of the right ear, which is quite lowset (white arrow) (A) and uvula bifida (white arrow) (B). Patient showing congenital migration of the scapula superiorly compared with the thoracic cage (white arrow) (C). Patient showing asymmetric thoracic wall: agenesis of the right pectoralis major muscle and hypoplastic right nipple (white arrow) (D).
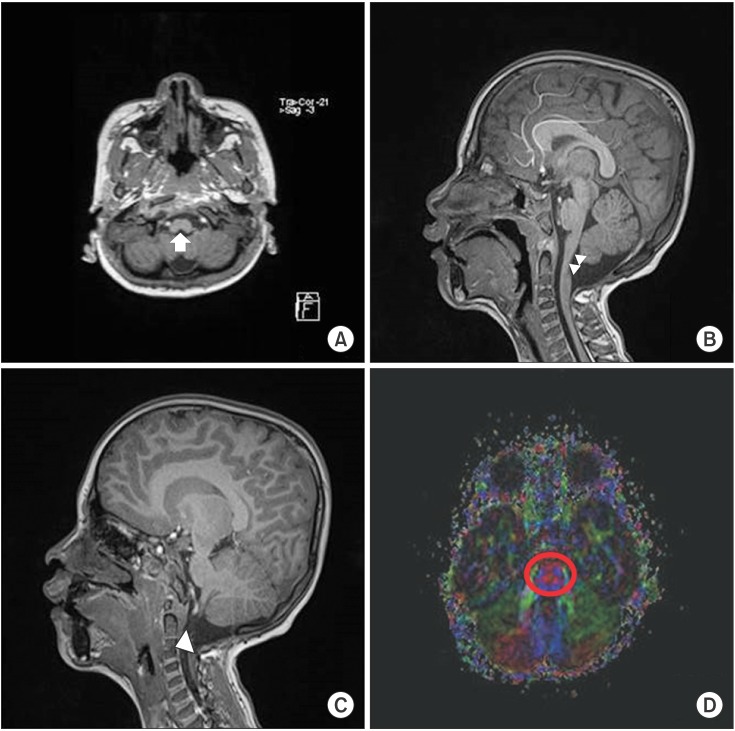
Fig. 2 T1-weighted transverse sagittal magnetic resonance image showing neuroschisis at the cervicomedullary junction (white arrow) (A) and split-cord malformation at the upper cervical cord (white arrowheads) (B). T1-weighted sagittal magnetic resonance image showing a cervical vertebral fusion at the level of C3–4 (white arrowhead) (C). The corticospinal tract (CST), central tegmental tract (CTT), and the transverse pontine fibers between CST and CTT on diffuse tensor imaging, with color fractional anisotropy maps in the red circle at the upper pontine level being normal (D).
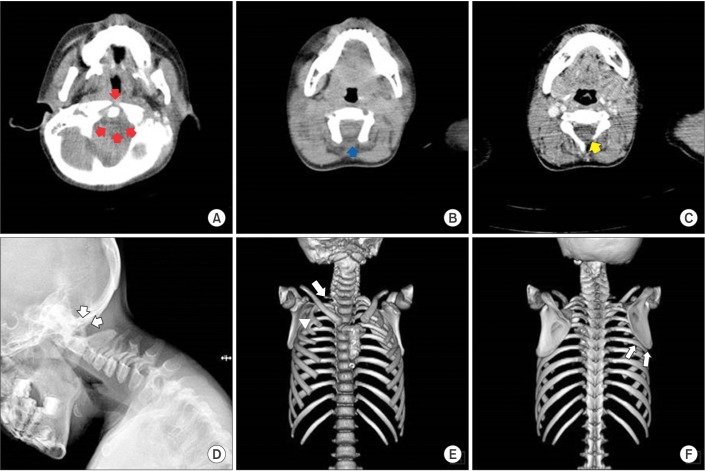
Fig. 3 Transverse c-spine computed tomography (CT) images showing aplasia of the C1 anterior and posterior arches (red arrows) (A), aplasia of the C2 posterior arch (blue arrow) (B), and the C3 left laminar aplasia (yellow arrow) (C). A simple lateral c-spine X-ray image showing the complete absence of the post arch of the C1 and C2 spine (white arrows) (D). 3D CT-reconstruction image showing right 1st rib agenesis (white arrow) and right 2nd and 3rd rib fusion (white arrowhead) (E). 3D CT-reconstruction image showing that the right scapula migrated superiorly compared with the left, and the inferior angle of the scapular blade is at the level of the 6th rib (white arrows) (F).
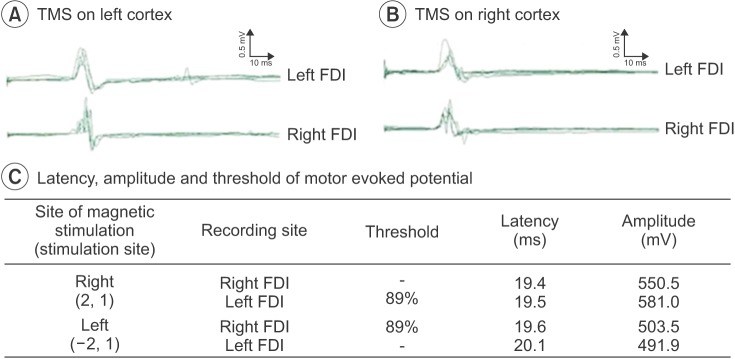
Fig. 4 Motor responses from transcranial magnetic stimulation (TMS) showing bilateral motor-evoked potentials from the first dorsal interosseous (FDI) muscles during left motor cortex stimulation (A). Motor responses of TMS showing bilateral motor-evoked potentials from the FDI muscles during right motor cortex stimulation (B). The best stimulation position was (–2,1) in the left cortex and (2,1) in the right cortex, and the threshold was 89% at both cortices (C).
Cited by 1 articles
-
Ten-Year Follow-Up of Transcranial Magnetic Stimulation Study in a Patient With Congenital Mirror Movements: A Case Report
Eu-Deum Kim, Gi-Wook Kim, Yu Hui Won, Myoung-Hwan Ko, Jeong-Hwan Seo, Sung-Hee Park
Ann Rehabil Med. 2019;43(4):524-529. doi: 10.5535/arm.2019.43.4.524.
Reference
-
1. Stewart FJ, Nevin NC, Brown S. Axial mesodermal dysplasia spectrum. Am J Med Genet. 1993; 45:426–429. PMID: 8465843.
Article2. Bergmann C, Zerres K, Peschgens T, Senderek J, Hornchen H, Rudnik-Schöneborn S. Overlap between VACTERL and hemifacial microsomia illustrating a spectrum of malformations seen in axial mesodermal dysplasia complex (AMDC). Am J Med Genet A. 2003; 121:151–155. PMID: 12910495.
Article3. Dias MS, Walker ML. The embryogenesis of complex dysraphic malformations: a disorder of gastrulation? Pediatr Neurosurg. 1992; 18:229–253. PMID: 1476931.
Article4. Royal SA, Tubbs RS, D'Antonio MG, Rauzzino MJ, Oakes WJ. Investigations into the association between cervicomedullary neuroschisis and mirror movements in patients with Klippel-Feil syndrome. AJNR Am J Neuroradiol. 2002; 23:724–729. PMID: 11950676.5. Preis S, Majewski F, Hantschmann R, Schumacher H, Lenard HG. Goldenhar, Mobius and hypoglossiahypodactyly anomalies in a patient: syndrome or association? Eur J Pediatr. 1996; 155:385–389. PMID: 8741036.6. Huang HT, Hwang CW, Lai PH, Chen CC. Mobius syndrome as a syndrome of rhombencephalic maldevelopment: a case report. Pediatr Neonatol. 2009; 50:36–38. PMID: 19326837.7. Foyaca-Sibat H, Ibanez-Valdes L. Klippel-Feil syndrome "plus". Internet J Intern Med. 2002; 4:1–6.8. Muroi A, Fleming KL, McComb JG. Split medulla in association with multiple closed neural tube defects. Childs Nerv Syst. 2010; 26:967–971. PMID: 20179945.
Article9. Webb BD, Frempong T, Naidich TP, Gaspar H, Jabs EW, Rucker JC. Mirror movements identified in patients with Moebius syndrome. Tremor Other Hyperkinet Mov (N Y). 2014; 4:256. PMID: 25120946.
Article10. Guebert GM, Rowe LJ, Yochum TR, Thompson JR, Maola CJ. Congenital anomalies and normal skeletal variants. In : Yochum TR, Rowe LJ, editors. Essentials of skeletal radiology. 1st ed. Baltimore: Lippincott Williams & Wilkins;1987. p. 95–168.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Anatomical Variations, Genitourinary Anomalies and Clinical Presentations in Obstructed Hemivagina and Ipsilateral Renal Anomaly Syndrome: Case Series
- A Case of Secondary Glaucoma combined with Mesodermal Dysgenesis of Anterior Segment
- Caudal Agenesis : Understanding the Base of the Wide Clinical Spectrum
- There cases of Hereditary Anhidrotic Ectodermal Dysplasia
- A Case of Malignant Mixed Mesodermal Tumor of the Ovary
