Solitary Rectal Ulcer Syndrome Mimicking Rectal Cancer
- Affiliations
-
- 1Department of Internal Medicine, Jeju National University School of Medicine, Jeju, Korea. songhj@jejunu.ac.kr
- 2Department of Surgery, Jeju National University School of Medicine, Jeju, Korea.
- 3Department of Radiology, Jeju National University School of Medicine, Jeju, Korea.
- 4Department of Pathology, Jeju National University School of Medicine, Jeju, Korea.
- KMID: 2152755
- DOI: http://doi.org/10.12771/emj.2016.39.1.28
Abstract
- Solitary rectal ulcer syndrome (SRUS) is a rare benign and chronic rectal disease that has a wide spectrum of clinical presentations and variable endoscopic findings. It is usually diagnosed by histopathological examination through biopsy. A 68-year-old man was referred to our hospital with anal pain and difficulty on bowel movement. Colonoscopy showed a hemorrhagic ulcerated mass in the rectum. All radiologic findings such as abdominopelvic computed tomography (CT), positron emission tomography-CT and magnetic resonance imaging were suspicious of rectal cancer. Although the patient underwent repeat endoscopic biopsy and one surgical biopsy, the results were not indicative of malignancy. Two months after conservative management, clinical symptoms and colonoscopic findings were markedly improved. Thus, we report this rare case of a 68-year-old man who had a central ulcerated mass that mimicked rectal cancer on gross colonoscopic and radiologic findings, representing an SRUS variant.
Keyword
MeSH Terms
Figure
-

Fig. 1 Endoscopic findings. (A) Colonoscopy shows a broad-based rectal lesion with irregular surface and hemorrhagic ulceration (arrow) (B) Rectal lesion is markedly improved with remnant ulcerative scarring two months later.
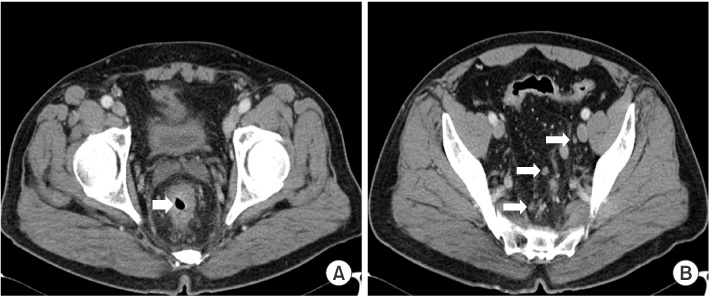
Fig. 2 Abdominopelvic computed tomography (CT) findings. (A) Enhanced CT image shows rectal wall thickening (arrow) and perirectal fatty infiltration. (B) Enlargement of multiple small mesocolic lymph nodes are observed (arrows).

Fig. 3 Radiologic findings. (A) Positron emission tomography-computed tomography shows intense fludeoxyglucose uptake (arrow) in rectum (maximum standardized uptake value, SUVmax 15.4), and (B) multiple enlarged mesocolic lymph nodes (arrows) with intense FDG uptake (SUV-max 8.1). (C) Magnetic resonance imaging reveals sagittal T2-weighted image of the pelvis showing irregular wall thickening of mid rectum (arrow).

Fig. 4 Pathologic findings. (A) There is surface erosion and ulceration, characterized by discontinuity of the epithelium with acute inflammation and exudates. The ulcerated rectal mucosa and submucosa reveals formation of granulation tissue characterized by an admixture of small vessels, numerous inflammatory cells, fibrin and edema (H&E, ×100). (B) Distorted crypts are strongly positive for cytokeratin staining (×100).
Reference
-
1. Abid S, Khawaja A, Bhimani SA, Ahmad Z, Hamid S, Jafri W. The clinical, endoscopic and histological spectrum of the solitary rectal ulcer syndrome: a single-center experience of 116 cases. BMC Gastroenterol. 2012; 12:72.2. Umar SB, Efron JE, Heigh RI. An interesting case of mistaken identity. Case Rep Gastroenterol. 2008; 2:308–313.3. Amaechi I, Papagrigoriadis S, Hizbullah S, Ryan SM. Solitary rectal ulcer syndrome mimicking rectal neoplasm on MRI. Br J Radiol. 2010; 83:e221–e224.4. Zhu QC, Shen RR, Qin HL, Wang Y. Solitary rectal ulcer syndrome: clinical features, pathophysiology, diagnosis and treatment strategies. World J Gastroenterol. 2014; 20:738–744.5. Gordon PH, Nivatvongs S. Solitary rectal ulcer syndrome of the rectum. In : Gordon PH, Nivatvongs S, editors. Principle and practice of surgery for the colon, rectum and anus. 2nd ed. St. Louis, MO: Quality Medical Publisher;1999. p. 1403–1409.6. Lawler LP, Fleshman JW. Solitary rectal ulcer, rectocele, hemorrhoids and pelvic pain. In : Pemberton JH, Swash M, Henry MM, editors. The pelvic floor, its function and disorders. London: WB Saunders;2002. p. 358–362.7. Chong VH, Jalihal A. Solitary rectal ulcer syndrome: characteristics, outcomes and predictive profiles for persistent bleeding per rectum. Singapore Med J. 2006; 47:1063–1068.8. Ingle SB, Patle YG, Murdeshwar HG, Hinge Ingle CR. An unusual case of solitary rectal ulcer syndrome mimicking inflammatory bowel disease and malignancy. Arab J Gastroenterol. 2012; 13:102.9. Perrakis E, Vezakis A, Velimezis G, Filippou D. Solitary rectal ulcer mimicking a malignant stricture. A case report. Rom J Gastroenterol. 2005; 14:289–291.10. Tjandra JJ, Fazio VW, Church JM, Lavery IC, Oakley JR, Milsom JW. Clinical conundrum of solitary rectal ulcer. Dis Colon Rectum. 1992; 35:227–234.11. Wong WM, Lai KC, Shek TW, Lam SK. Self-inflicted rectal ulcer with exuberant granulation tissue: a lesion that mimics carcinoma. Gastrointest Endosc. 2002; 55:951–952.12. Al-Brahim N, Al-Awadhi N, Al-Enezi S, Alsurayei S, Ahmad M. Solitary rectal ulcer syndrome: a clinicopathological study of 13 cases. Saudi J Gastroenterol. 2009; 15:188–192.13. Park HJ, Kim WH, Woo JS, Han KH, Lee SI, Park IS, et al. Solitary rectal ulcer syndrome. Yonsei Med J. 1994; 35:223–230.14. Blanco F, Frasson M, Flor-Lorente B, Minguez M, Esclapez P, Garcia-Granero E. Solitary rectal ulcer: ultrasonographic and magnetic resonance imaging patterns mimicking rectal cancer. Eur J Gastroenterol Hepatol. 2011; 23:1262–1266.15. Delgado J, Delgado B, Sztarkier I, Sperber AD, Walfisch S. A solitary rectal ulcer mimicking rectal cancer. Gastrointest Endosc. 2005; 62:309.
