Korean J Obstet Gynecol.
2012 Aug;55(8):614-617. 10.5468/KJOG.2012.55.8.614.
Polypoid huge ovarian mass manifesting as massive ascites in a young woman
- Affiliations
-
- 1Department of Obstetrics and Gynecology, Ewha Womans University School of Medicine, Seoul, Korea. sarahmd@ewha.ac.kr
- KMID: 2078116
- DOI: http://doi.org/10.5468/KJOG.2012.55.8.614
Abstract
- In young aged female patients complaining of abdominal distension, we have to consider the possibility of pelvic mass of gynecologic origin even if the imaging study suggest massive ascites with bilateral normal ovaries, especially in whom without underlying medical disease or symptoms of ascites. Polypoid huge ovarian mass with thin wall could manifest as massive ascites as in this case. Following careful counseling with patient, the diagnostic laparoscopy could be a good option for early diagnosis and treatment in such a case, instead of performing numerous diagnostic work-up to find out the medical disease causing massive ascites.
Keyword
Figure
-

Fig. 1 Abdomino-pelvic computed tomography suggesting normal both ovaries without adnexal mass and massive ascites of unknown origin filling the entire abdomino-pelvic cavity.
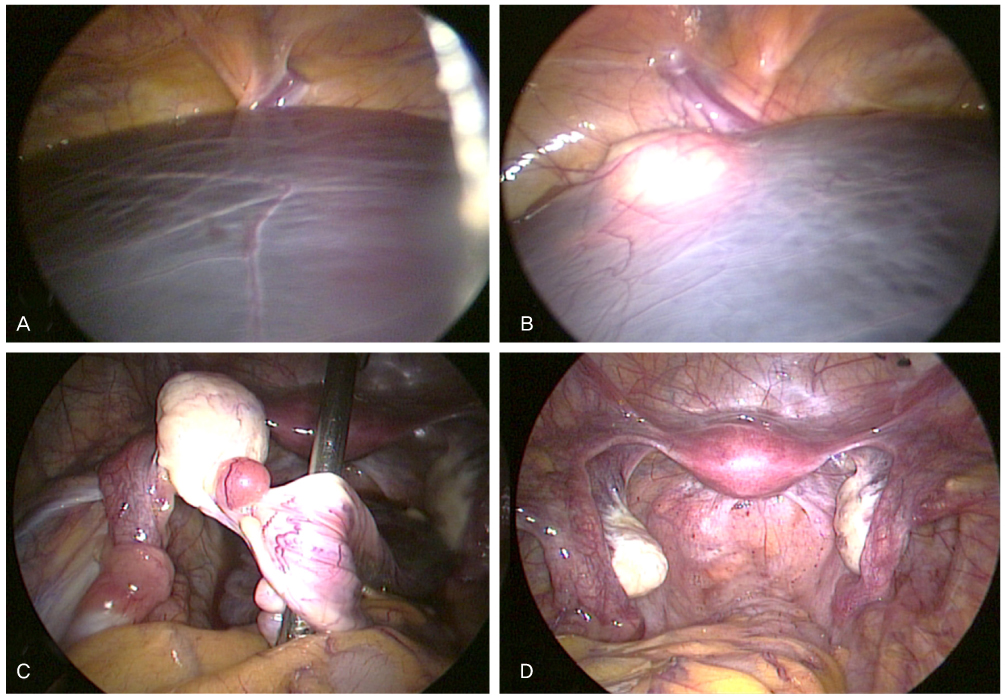
Fig. 2 Diagnostic laparoscopic findings (A, B) Huge thin walled cystic mass filling entire abdomino-pelvic cavity and left ovary. (C) A mass with polypoid outgrowth from left ovary. (D) Postoperative state showing normal bilateral ovaries and tubes.

Fig. 3 Microscopic photograph of the polypoid huge ovarian tumor. (A) Tumor consisting of epithelial lining composed of columnar and cuboidal cell (H&E, ×40). (B) Cyst-lining cells without nuclear atypia, stromal invasion, or mitosis (H&E, ×400).
Reference
-
1. Göçmen A, Atak T, Uçar M, Sanlikal F. Laparoscopy-assisted cystectomy for large adnexal cysts. Arch Gynecol Obstet. 2009. 279:17–22.2. Gungor T, Kanat-Pektas M, Ozat M, Zayifoglu Karaca M. A systematic review: endometriosis presenting with ascites. Arch Gynecol Obstet. 2011. 283:513–518.3. Le T, Giede C, Salem S, Lefebvre G, Rosen B, Bentley J, et al. Initial evaluation and referral guidelines for management of pelvic/ovarian masses. J Obstet Gynaecol Can. 2009. 31:668–680.4. Onderoglu LS, Gültekin M, Dursun P, Karcaaltincaba M, Usubutun A, Akata D, et al. Bilateral ovarian fibromatosis presenting with ascites and hirsutism. Gynecol Oncol. 2004. 94:223–225.5. Chalermchockcharoenkit A, Chaisilwattana P, Ruangvutilert P. Laparoscopic cystectomy of an ovarian mucinous cystadenoma in a 12-year-old girl: a possible role of operative laparoscopy for a huge benign adnexal mass. J Med Assoc Thai. 2004. 87:113–118.6. Abu J, Brown L, Ireland D, Sizeland E. Mesovarian hemangioma presenting as massive ascites, pelvic mass, and elevated CA125. Int J Gynecol Cancer. 2006. 16:Suppl 1. 412–414.7. Păun I, Mogoş D, Păun M, Teodorescu M, Florescu M, Tenovici M, et al. Diseases mimicking advanced-stage epithelial ovarian cancer. Chirurgia (Bucur). 2010. 105:541–544.8. Ofluoglu R, Güler M, Unsal E, Kiliç N, Capan N. Malignity-like peritoneal tuberculosis associated with abdominal mass, ascites and elevated serum Ca125 level. Acta Chir Belg. 2009. 109:71–74.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Massive Ovarian Edema
- Meigs' Syndrome with Elevated Cancer Antigen 125
- Adult granulosa cell tumor presenting with massive ascites, elevated CA-125 level, and low 18F-fluorodeoxyglucose uptake on positron emission tomography/computed tomography
- An Ovarian Steroid Cell Tumor Causing Virilization and Massive Ascites
- A Case of Benign Ovarian Steroid Cell Tumor with Huge Ascites and Elevated Serum CA125
