Intest Res.
2015 Oct;13(4):332-338. 10.5217/ir.2015.13.4.332.
Clinical Features and Prognosis of Resectable Primary Colorectal Signet-Ring Cell Carcinoma
- Affiliations
-
- 1Department of Gastroenterology, University of Ulsan College of Medicine, Asan Medical Center, Seoul, Korea. dhyang@amc.seoul.kr
- 2Department of Pathology, University of Ulsan College of Medicine, Asan Medical Center, Seoul, Korea.
- 3Department of Colon and Rectal Surgery, University of Ulsan College of Medicine, Asan Medical Center, Seoul, Korea. csyu@amc.seoul.kr
- KMID: 2070749
- DOI: http://doi.org/10.5217/ir.2015.13.4.332
Abstract
- BACKGROUND/AIMS
We attempted to investigate the prognosis of signet-ring cell carcinoma (SRC) patients who underwent curative surgery by comparing them with age-, sex-, and stage-matched non-mucinous adenocarcinoma (NMAC) patients.
METHODS
Between January 2003 and December 2011, 19 patients with primary SRC of the colorectum underwent curative surgery. Four SRC patients under the age of 40 were excluded, and the clinicopathological data of 15 patients (7 men; median age, 56 years) were reviewed and compared with the data of 75 NMAC patients matched by age, sex, and pathologic stage.
RESULTS
The median follow-up duration was 30.1 months for the SRC group and 43.7 months for the NMAC group (P=0.141). Involvement of the left side of the colon (73.3% vs. 26.7%, P=0.003) and infiltrative lesions such as Borrmann types 3 and 4 (85.7% vs. 24.0%, P=0.001) were more common in the SRC group than in the NMAC group. The five-year overall survival rate was significantly lower for patients with SRC than for those with NMAC (46.0% vs. 88.7%, hazard ratio, 6.99; 95% confidence interval, 2.33-20.95, P=0.001).
CONCLUSIONS
Patients with even resectable primary colorectal SRC had a poorer prognosis than age-, sex-, and stage-matched colorectal NMAC patients.
Keyword
MeSH Terms
Figure
-
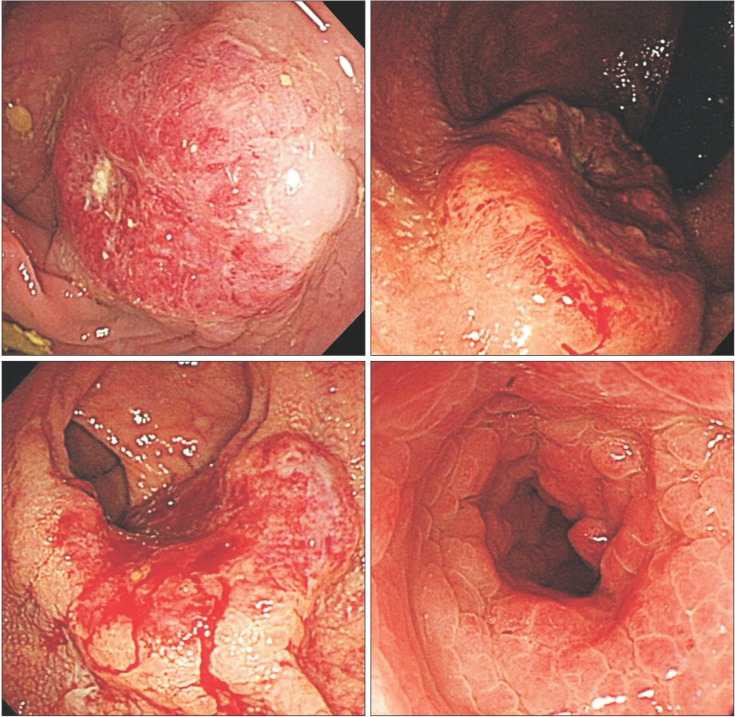
Fig. 1 Borrmann classification of colorectal cancer. (A) A case of Bormann type I (polypoid type) non-mucinous adenocarcinoma; (B) A case of Bormann type II (ulcerofungating type) signet-ring cell carcinoma (SRC); (C) A case of Bormann type III (ulceroinfiltrative type) SRC; and (D) A case of Bormann type IV (infiltrative type) SRC.
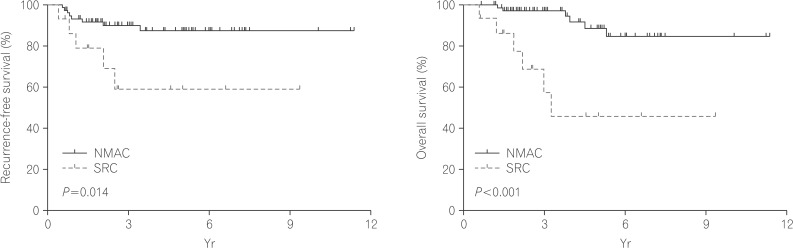
Fig. 2 Kaplan-Meier survival curves comparing the recurrence-free (A) and overall survival (B) of patients with signet-ring-cell carcinoma (SRC) and patients with non-mucinous adenocarcinoma (NMAC) (log-rank test).
Reference
-
1. Siegel R, Naishadham D, Jemal A. Cancer statistics, 2013. CA Cancer J Clin. 2013; 63:11–30. PMID: 23335087.
Article2. Sung JJ, Lau JY, Goh KL, Leung WK. Asia Pacific Working Group on Colorectal Cancer. Increasing incidence of colorectal cancer in Asia: implications for screening. Lancet Oncol. 2005; 6:871–876. PMID: 16257795.
Article3. Byeon JS, Yang SK, Kim TI, et al. Colorectal neoplasm in asymptomatic Asians: a prospective multinational multicenter colonoscopy survey. Gastrointest Endosc. 2007; 65:1015–1022. PMID: 17531636.
Article4. Secco GB, Fardelli R, Campora E, et al. Primary mucinous adenocarcinomas and signet-ring cell carcinomas of colon and rectum. Oncology. 1994; 51:30–34. PMID: 8265100.
Article5. Messerini L, Palomba A, Zampi G. Primary signet-ring cell carcinoma of the colon and rectum. Dis Colon Rectum. 1995; 38:1189–1192. PMID: 7587762.
Article6. Tung SY, Wu CS, Chen PC. Primary signet ring cell carcinoma of colorectum: an age- and sex-matched controlled study. Am J Gastroenterol. 1996; 91:2195–2199. PMID: 8855747.7. Nozoe T, Anai H, Nasu S, Sugimachi K. Clinicopathological characteristics of mucinous carcinoma of the colon and rectum. J Surg Oncol. 2000; 75:103–107. PMID: 11064389.
Article8. Chen JS, Hsieh PS, Hung SY, et al. Clinical significance of signet ring cell rectal carcinoma. Int J Colorectal Dis. 2004; 19:102–107. PMID: 14752674.
Article9. Wu CS, Tung SY, Chen PC, Kuo YC. Clinicopathological study of colorectal mucinous carcinoma in Taiwan: a multivariate analysis. J Gastroenterol Hepatol. 1996; 11:77–81. PMID: 8672747.
Article10. Kang H, O'Connell JB, Maggard MA, Sack J, Ko CY. A 10-year outcomes evaluation of mucinous and signet-ring cell carcinoma of the colon and rectum. Dis Colon Rectum. 2005; 48:1161–1168. PMID: 15868237.
Article11. Hyngstrom JR, Hu CY, Xing Y, et al. Clinicopathology and outcomes for mucinous and signet ring colorectal adenocarcinoma: analysis from the National Cancer Data Base. Ann Surg Oncol. 2012; 19:2814–2821. PMID: 22476818.
Article12. Börger ME, Gosens MJ, Jeuken JW, et al. Signet ring cell differentiation in mucinous colorectal carcinoma. J Pathol. 2007; 212:278–286. PMID: 17471475.
Article13. Chen JS, Hsieh PS, Chiang JM, et al. Clinical outcome of signet ring cell carcinoma and mucinous adenocarcinoma of the colon. Chang Gung Med J. 2010; 33:51–57. PMID: 20184795.14. Mizushima T, Nomura M, Fujii M, et al. Primary colorectal signet-ring cell carcinoma: clinicopathological features and postoperative survival. Surg Today. 2010; 40:234–238. PMID: 20180076.
Article15. Song W, Wu SJ, He YL, et al. Clinicopathologic features and survival of patients with colorectal mucinous, signet-ring cell or non-mucinous adenocarcinoma: experience at an institution in southern China. Chin Med J (Engl). 2009; 122:1486–1491. PMID: 19719934.16. Pyo SH, Byeon JS, Myung SJ, et al. Clinical and Colonoscopic Characteristics of Primary Signet Ring Cell Carcinoma in Colorectum. Korean J Gastrointest Endosc. 2006; 33:278–284.17. Nissan A, Guillem JG, Paty PB, Wong WD, Cohen AM. Signetring cell carcinoma of the colon and rectum: a matched control study. Dis Colon Rectum. 1999; 42:1176–1180. PMID: 10496558.
Article18. Makino T, Tsujinaka T, Mishima H, et al. Primary signet-ring cell carcinoma of the colon and rectum: report of eight cases and review of 154 Japanese cases. Hepatogastroenterology. 2006; 53:845–849. PMID: 17153438.19. Lee WS, Chun HK, Lee WY, et al. Treatment outcomes in patients with signet ring cell carcinoma of the colorectum. Am J Surg. 2007; 194:294–298. PMID: 17693269.
Article20. Sung CO, Seo JW, Kim KM, Do IG, Kim SW, Park CK. Clinical significance of signet-ring cells in colorectal mucinous adenocarcinoma. Mod Pathol. 2008; 21:1533–1541. PMID: 18849918.
Article21. Ooi BS, Ho YH, Eu KW, Seow Choen F. Primary colorectal signet-ring cell carcinoma in Singapore. ANZ J Surg. 2001; 71:703–706. PMID: 11906382.
Article22. Kim KH, Yang SS, Yoon YS, Lim SB, Yu CS, Kim JC. Validation of the seventh edition of the American Joint Committee on Cancer tumor-node-metastasis (AJCC TNM) staging in patients with stage II and stage III colorectal carcinoma: analysis of 2511 cases from a medical centre in Korea. Colorectal Dis. 2011; 13:e220–e226. PMID: 21689314.
Article23. Park HC, Shin A, Kim BW, et al. Data on the characteristics and the survival of korean patients with colorectal cancer from the Korea central cancer registry. Ann Coloproctol. 2013; 29:144–149. PMID: 24032114.
Article24. Kakar S, Smyrk TC. Signet ring cell carcinoma of the colorectum: correlations between microsatellite instability, clinicopathologic features and survival. Mod pathol. 2005; 18:244–249. PMID: 15492759.
Article25. Kazama Y, Watanabe T, Kanazawa T, Tada T, Tanaka J, Nagawa H. Mucinous carcinomas of the colon and rectum show higher rates of microsatellite instability and lower rates of chromosomal instability: a study matched for T classification and tumor location. Cancer. 2005; 103:2023–2029. PMID: 15812832.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Cytologic Features of Signet Ring Cell Carcinoma of the Uterine Cervix: A Report of Two Cases
- Characteristics of Primary Colorectal Signet Ring Cell Carcinoma
- Primary Signet Ring Cell Carcinoma of the Colon and Rectum
- Signet Ring Cell Carcinoma of the Prostate A report of two cases
- Primary Signet Ring Cell Carcinoma of the Urinary Bladder
