Pediatr Gastroenterol Hepatol Nutr.
2015 Sep;18(3):160-167. 10.5223/pghn.2015.18.3.160.
Efficacy and Safety of Low Dose Ketamine and Midazolam Combination for Diagnostic Upper Gastrointestinal Endoscopy in Children
- Affiliations
-
- 1Department of Pediatric Gastroenterology Hepatology and Nutrition, Faculty of Medicine, Karadeniz Technical University, Trabzon, Turkey. ulasemre@hotmail.com
- KMID: 2068792
- DOI: http://doi.org/10.5223/pghn.2015.18.3.160
Abstract
- PURPOSE
We aimed to analyze the effectiveness and safety of low-dose midazolam and ketamine combination for upper gastrointestinal endoscopy (UGIE) in children.
METHODS
The study included the children (n=425, 10.78+/-3.81 years) who underwent UGIE for diagnostic purpose during 1 year period. All children were sedated with low dose midazolam (0.1 mg/kg) and ketamine (0.5 mg/kg) intravenously. Effectiveness of the sedation and complications during the procedure and recovery period were recorded.
RESULTS
Endoscopic procedure was successfully completed in 414 patients (97.4%; 95% confidence interval, 95.8-98.9). Mean+/-standard deviation (SD) duration of procedure was 6.36+/-1.64 minutes (median, 6.0 minutes; range, 4-12 minutes). Minor complications occurred during the procedure in 39.2% of the patients. The most common complication was increased oral secretion (33.1%). No major complications were observed in any patient. Age and Ramsay sedation scores of patients with complications during the procedure were lower than the others (9.49+/-4.05 years vs. 11.61+/-3.43 years, p=0.002 and 2.10+/-1.46 vs. 4.37+/-1.16, p=0.001). Mean recovery time was 22 minutes (range, 10-90 minutes; mean+/-SD, 25+/-12.32 minutes). Minor complications developed during recovery in 60.1% of the patients. The most common complication was transient double vision (n=127, 30.7%). Emergence reaction was observed in 5 patients (1.2%).
CONCLUSION
The procedure was completed with high level of success without any major complication in our study. Combination of low-dose midazolam and ketamine is a suitable sedation protocol for pediatric endoscopists in UGIE.
Keyword
MeSH Terms
Figure
-
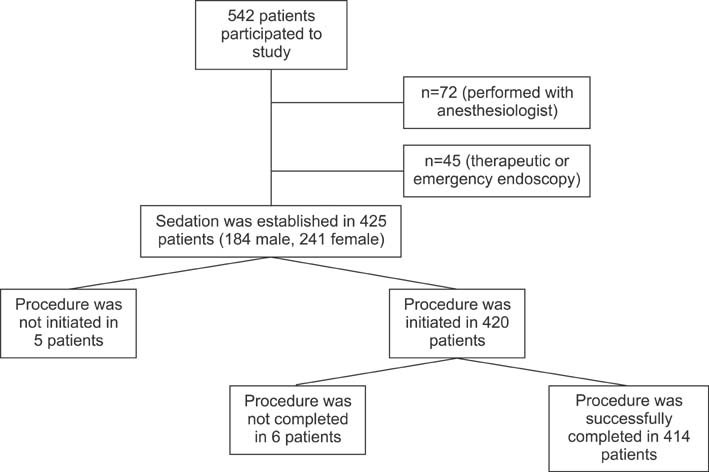
Fig. 1 Study protocol.

Fig. 2 Ramsay sedation score (RSS) of the patients.
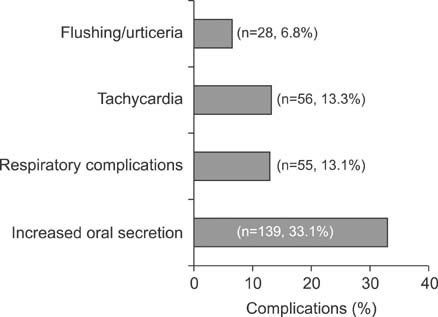
Fig. 3 Frequency of complications during the procedure.

Fig. 4 Frequency of complications during the recovery.
Cited by 1 articles
-
Propofol with and without Midazolam for Diagnostic Upper Gastrointestinal Endoscopies in Children
Ulas Emre Akbulut, Seyfi Kartal, Ufuk Dogan, Gulgun Elif Akcali, Serap Kalayci, Hulya Kirci
Pediatr Gastroenterol Hepatol Nutr. 2019;22(3):217-224. doi: 10.5223/pghn.2019.22.3.217.
Reference
-
1. Schwarz SM, Lightdale JR, Liacouras CA. Sedation and anesthesia in pediatric endoscopy: one size does not fit all. J Pediatr Gastroenterol Nutr. 2007; 44:295–297.
Article2. Krauss B, Green SM. Procedural sedation and analgesia in children. Lancet. 2006; 367:766–780.
Article3. Martinez JL, Sutters KA, Waite S, Davis J, Medina E, Montano N, et al. A comparison of oral diazepam versus midazolam, administered with intravenous meperidine, as premedication to sedation for pediatric endoscopy. J Pediatr Gastroenterol Nutr. 2002; 35:51–58.
Article4. Malamed SF. Pharmacology. In : Malamed SF, editor. Sedation A guide to patient management. Missouri: Mosby Company;1989. p. 330–379.5. Reves JG, Glass PSA, Lubarsky DA. Nonbarbiturate intravenous anesthetics. In : Miller RD, Cucchiara RF, editors. Anesthesia. 5th ed. Philadelphia: Churchill Livingstone;2000. p. 228–272.6. Verhage J, Mulder CJ, Willekens FL. Intravenous midazolam sedation in pediatric diagnostic upper digestive endoscopy. A prospective study in a general hospital. Rom J Gastroenterol. 2003; 12:273–276.7. Mamula P, Markowitz JE, Neiswender K, Zimmerman A, Wood S, Garofolo M, et al. Safety of intravenous midazolam and fentanyl for pediatric GI endoscopy: prospective study of 1578 endoscopies. Gastrointest Endosc. 2007; 65:203–210.
Article8. Moore KA, Sklerov J, Levine B, Jacobs AJ. Urine concentrations of ketamine and norketamine following illegal consumption. J Anal Toxicol. 2001; 25:583–588.
Article9. Gilger MA, Spearman RS, Dietrich CL, Spearman G, Wilsey MJ Jr, Zayat MN. Safety and effectiveness of ketamine as a sedative agent for pediatric GI endoscopy. Gastrointest Endosc. 2004; 59:659–663.
Article10. Kirberg A, Sagredo R, Montalva G, Flores E. Ketamine for pediatric endoscopic procedures and as a sedation complement for adult patients. Gastrointest Endosc. 2005; 61:501–502.
Article11. Motamed F, Aminpour Y, Hashemian H, Soltani AE, Najafi M, Farahmand F. Midazolam-ketamine combination for moderate sedation in upper GI endoscopy. J Pediatr Gastroenterol Nutr. 2012; 54:422–426.
Article12. White PF, Way WL, Trevor AJ. Ketamine--its pharmacology and therapeutic uses. Anesthesiology. 1982; 56:119–136.
Article13. Reich DL, Silvay G. Ketamine: an update on the first twenty-five years of clinical experience. Can J Anaesth. 1989; 36:186–197.
Article14. Green SM, Johnson NE. Ketamine sedation for pediatric procedures: part 2, review and implications. Ann Emerg Med. 1990; 19:1033–1046.
Article15. Green SM, Roback MG, Kennedy RM, Krauss B. Clinical practice guideline for emergency department ketamine dissociative sedation: 2011 update. Ann Emerg Med. 2011; 57:449–461.
Article16. Lowrie L, Weiss AH, Lacombe C. The pediatric sedation unit: a mechanism for pediatric sedation. Pediatrics. 1998; 10:E30.
Article17. Green SM, Li J. Ketamine in adults: what emergency physicians need to know about patient selection and emergence reactions. Acad Emerg Med. 2000; 7:278–281.
Article18. Tolia V, Peters JM, Gilger MA. Sedation for pediatric endoscopic procedures. J Pediatr Gastroenterol Nutr. 2000; 30:477–485.
Article19. Miqdady MI, Hayajneh WA, Abdelhadi R, Gilger MA. Ketamine and midazolam sedation for pediatric gastrointestinal endoscopy in the Arab world. World J Gastroenterol. 2011; 17:3630–3635.
Article20. Brecelj J, Trop TK, Orel R. Ketamine with and without midazolam for gastrointestinal endoscopies in children. J Pediatr Gastroenterol Nutr. 2012; 54:748–752.
Article21. Chong JH, Chew SP, Ang AS. Is prophylactic atropine necessary during ketamine sedation in children? J Paediatr Child Health. 2013; 49:309–312.
Article22. Hofley MA, Hofley PM, Keon TP, Gallagher PR, Poon C, Liacouras CA. A placebo-controlled trial using intravenous atropine as an adjunct to conscious sedation in pediatric esophagogastroduodenoscopy. Gastrointest Endosc. 1995; 42:457–460.
Article23. Green SM, Roback MG, Krauss B, Brown L, McGlone RG, Agrawal D, et al. Emergency Department Ketamine Meta-Analysis Study Group. Predictors of emesis and recovery agitation with emergency department ketamine sedation: an individual-patient data meta-analysis of 8,282 children. Ann Emerg Med. 2009; 54:171–180.
Article24. Rafeey M, Ghojazadeh M, Feizo Allah Zadeh H, Majidi H. Use of oral midazolam in pediatric upper gastrointestinal endoscopy. Pediatr Int. 2010; 52:191–195.
Article25. Piraccini E, Albarello R, Biagini C, Novi A, Agnoletti V, Gambale G. Spinal anesthesia plus ketamine-midazolam sedation for pediatric orthopedic surgery in a developing country. HSR Proc Intensive Care Cardiovasc Anesth. 2012; 4:176–178.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Vital Sign and Sedative Effect of Midazolam for Conscious Sedation during Upper Gastrointestinal Endoscopy
- Midazolam as Premedication for Upper Gastrointestinal Endoscopy
- Efficacy and Safety of Etomidate in Comparison with Propofol or Midazolam as Sedative for Upper Gastrointestinal Endoscopy
- The Effects of the Combination of Ketamine and Midazolam for Sedation during Epidural Anesthesia
- Effectiveness of Flumazenil against Midazolam as Premedication for Upper Gastrointestinal Endoscopy
