Probable Isolated Hypertensive Brainstem Encephalopathy Combined with Intracerebral Hemorrhage: a Case Report
- Affiliations
-
- 1Department of Radiology, Dongguk University International Hospital, Dongguk University, Goyang-si, Korea.
- 2Department of Radiology, Korea University Ansan Hospital, Ansan-si, Korea. seohs@korea.ac.kr
- 3Department of Neurology, Dongguk University International Hospital, Dongguk University, Goyang-si, Korea.
- KMID: 1999926
- DOI: http://doi.org/10.13104/jksmrm.2014.18.3.258
Abstract
- Hypertensive encephalopathy and basal ganglia intracerebral hemorrhage (ICH) are a medical emergency caused by a sudden elevation of systemic blood pressure. Although the relationship between hypertensive encephalopathy and large ICH has not been clarified yet, Cushing reflex in acute elevations of ICP due to large ICH may induce or aggravate hypertensive encephalopathy. We report a rare case of isolated hypertensive brainstem encephalopathy combined with hypertensive ICH.
MeSH Terms
Figure
-
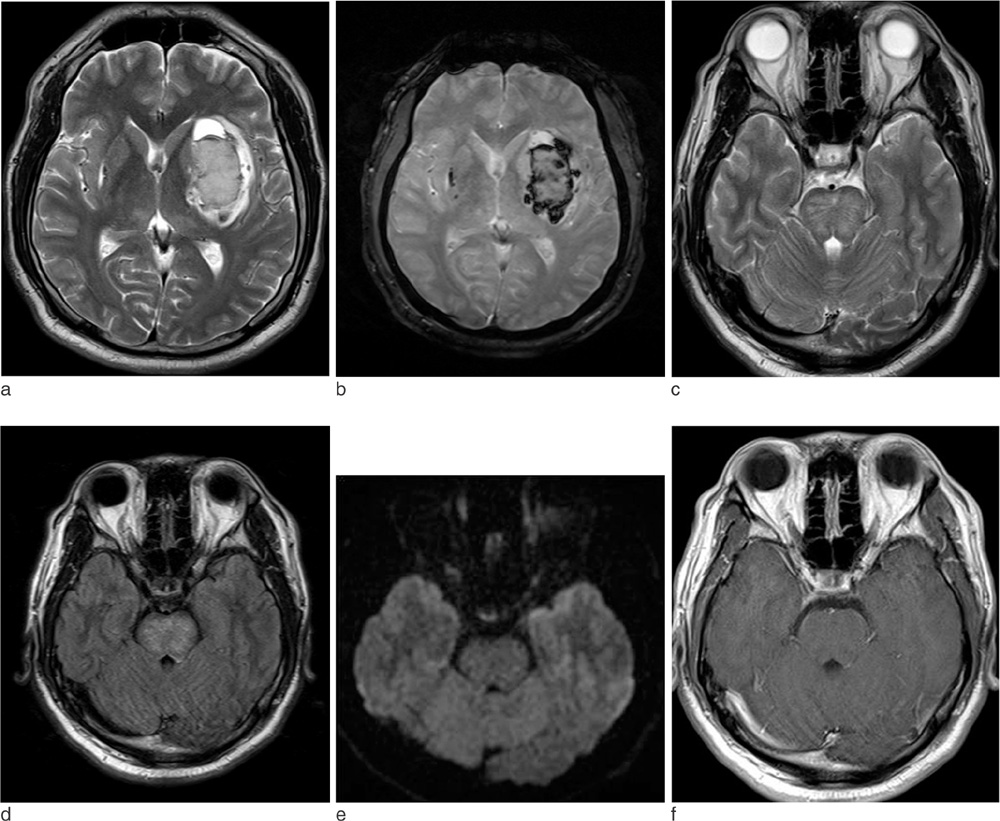
Fig. 1 MR images at the time of admission. (a) Transverse T2-weighted and (b) T2*-gradient echo MR images at the basal ganglia show a large acute stage hemorrhage in the left basal ganglia with mild perilesional edema. Another small hemorrhage is noted in the right basal ganglia. There is no abnormal signal intensity in the parieto-occipital areas on the T2-weighted image. (c) Transverse T2-weighted MR and (d) FLAIR images at the pons show diffuse hyperintensity in the pons with sparing of the peripheral areas. (e) This lesion shows no abnormal signal intensity on diffusion-weighted image. (f) There is no enhancement on contrast enhanced T1-weighted image.
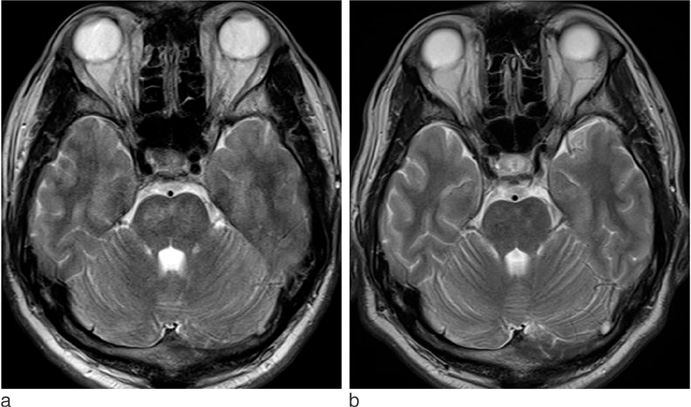
Fig. 2 Follow-up MR images on 6 days and 3 weeks later. (a) Transverse T2-weighted MR image on 6 days later shows an improved hyperintense lesion in pons but there is small residual patchy lesion. (b) Transverse T2-weighted MR image on 3 weeks later shows a complete improvement of pontine hyperintensity.
Reference
-
1. Morello F, Marino A, Cigolini M, Cappellari F. Hypertensive brain stem encephalopathy: clinical silent massive edema of the pons. Neurol Sci. 2001; 22:317–320.2. de Seze J, Mastain B, Stojkovic T, et al. Unusual MR findings of the brain stem in arterial hypertension. AJNR Am J Neuroradiol. 2000; 21:391–394.3. Hinchey J, Chaves C, Appignani B, et al. A reversible posterior leukoencephalopathy syndrome. N Engl J Med. 1996; 334:494–500.4. Bhagavati S, Chum F, Choi J. Hypertensive encephalopathy presenting with isolated brainstem and cerebellar edema. J Neuroimaging. 2008; 18:454–456.5. Chang GY, Keane JR. Hypertensive brainstem encephalopathy: three cases presenting with severe brainstem edema. Neurology. 1999; 53:652–654.6. Chang GY, Keane JR. Hypertensive brain stem encephalopathy. AJNR Am J Neuroradiol. 2000; 21(7):1366.7. Thambisetty M, Biousse V, Newman NJ. Hypertensive brainstem encephalopathy: clinical and radiographic features. J Neurol Sci. 2003; 208:93–99.8. Kang BW, Bae YJ, Cheon WH, Park SP, Suh CK. Two cases of hypertensive brainstem encephalopathy. J Korean Neurol Assoc. 2003; 21:535–538.9. Gamanagatti S, Subramanian S. Hypertensive encephalopathy: isolated pons involvement mimicking central pontine myelinolysis. Korean J Radiol. 2006; 7:218–219.10. Jones JV. Differentiation and investigation of primary versus secondary hypertension (Cushing reflex). Am J Cardiol. 1989; 63:10C–13C.11. Fodstad H, Kelly PJ, Buchfelder M. History of the Cushing reflex. Neurosurgery. 2006; 59:1132–1137.12. Casey SO, Truwit CL. Pontine reversible edema: a newly recognized imaging variant of hypertensive encephalopathy. AJNR Am J Neuroradiol. 2000; 21:243–245.13. Kumai Y, Kazunori T, Kenichiro F, Setsuro I. Hypertensive encephalopathy extending into the whole brainstem and deep structures. Hypertens Res. 2002; 25:797–800.14. Ay H, Buonanno FS, Schaefer PW, et al. Posterior leukoencephalopathy without severe hypertension: utility of diffusionweighted MRI. Neurology. 1998; 51:1369–1376.15. Doi Y, Kimura F, Fujuyama T, et al. Hypertensive brainstem encephalopathy without parieto-occipital lesion-two case reports. Neurol Med Chir (Tokyo). 2006; 46:75–77.16. Lee S, Cho BK, Kim H. Hypertensive encephalopathy with reversible brainstem edema. J Korean Neurosurg Soc. 2013; 54:139–141.17. Mccormick WF, Rosenfield DB. Massive brain hemorrhage: a review of 144 cases and an examination of their causes. Stroke. 1973; 4:946–954.18. de Morais BS, Carneiro FS, Araújo Rde M, Araújo GF, de Oliveira RB. Central pontine myelinolysis after liver transplantation: is sodium the only villain? Case report. Rev Bras Anestesiol. 2009; 59:344–349.19. Lampl C, Yazdi K. Central pontine myelinolysis. Eur Neurol. 2002; 47:3–10.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Two Cases of Hypertensive Brainstem Encephalopathy
- Two Cases of Hypertensive Encephalopathy Involving the Brainstem
- Hypertensive Brainstem Encephalopathy Combined with Acute Ischemic Stroke
- Severe Posterior Reversible Encephalopathy in Pheochromocytoma: Importance of Susceptibility-Weighted MRI
- Predominant Hypertensive Brainstem Encephalopathy with Supratentorial Involvement: Case Report and Literature Review
