Severe Posterior Reversible Encephalopathy in Pheochromocytoma: Importance of Susceptibility-Weighted MRI
- Affiliations
-
- 1Department of Radiology, Bezmialem Vakif University School of Medicine, Istanbul 34093, Turkey. asli_serter@yahoo.com
- KMID: 1711446
- DOI: http://doi.org/10.3348/kjr.2013.14.5.849
Abstract
- Pheochromocytoma is a rare cause of hypertension in children. Hypertension is one of the common reasons of posterior reversible encephalopathy. Intracerebral hemorrhage is a serious and unexpected complication of hypertensive encephalopathy due to pheochromocytoma, and very rarely seen in the childhood. Intracerebral hemorrhages should be searched if there are hypertensive reversible signal changes on the brain. Susceptibility weighted imaging (SWI) is a more sensitive method than conventional MRI when demonstrating cerebral microhemorrhagic foci. This is the first report of SWI findings on intracerebral hemorrhages in basal ganglia, brain stem and periventricular white matter due to hypertensive encephalopathy in a child with pheochromocytoma.
MeSH Terms
Figure
-
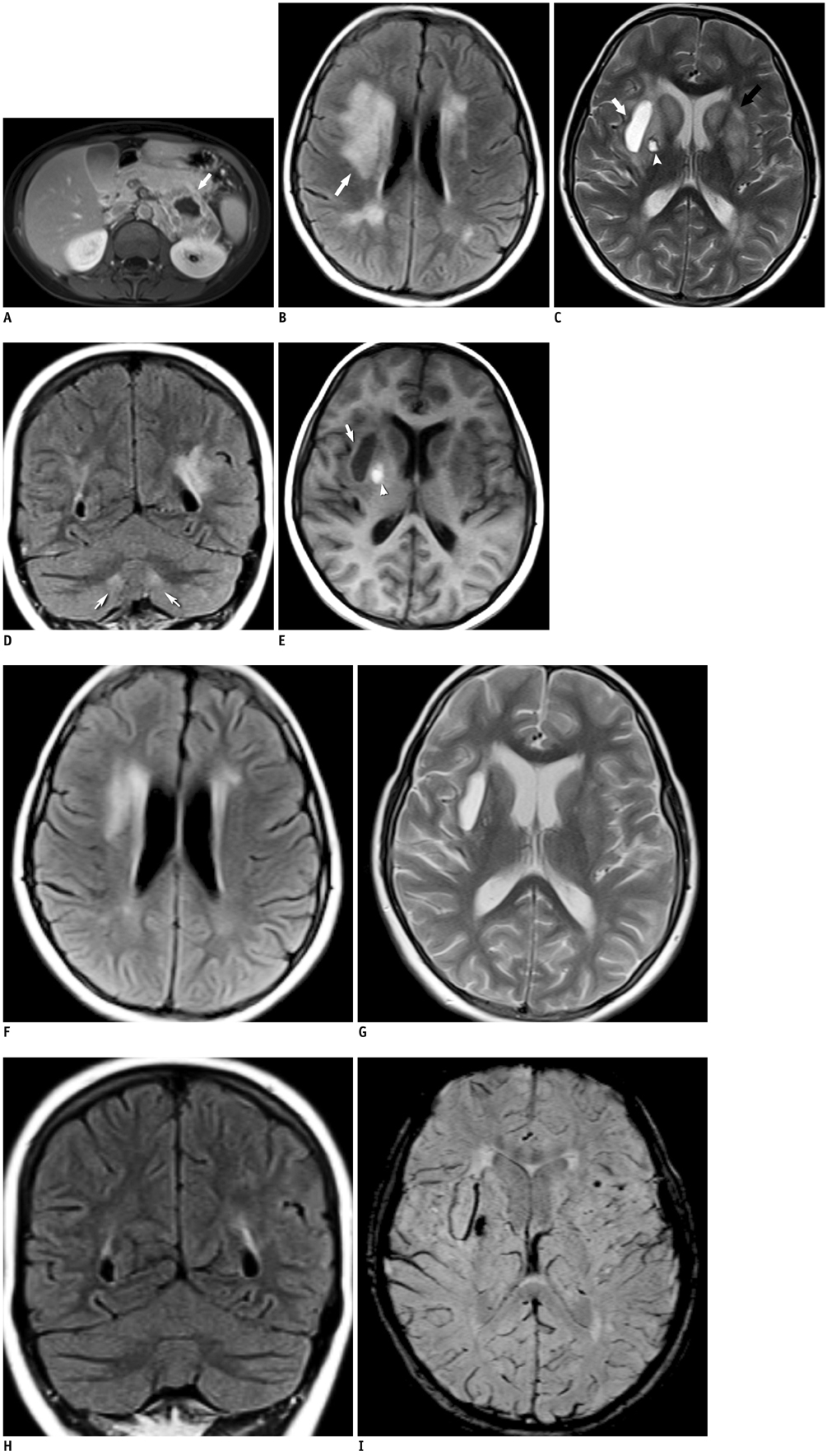
Fig. 1 MR appearance of hypertensive encephalopathy before treatment in patient with left surrenal pheochromocytoma. A. Axial contrast enhanced T1-weighted MRI shows large heterogeneous enhancing mass with central cystic necrotic area on left adrenal gland (arrow). B-E. Axial FLAIR (B), T2-weighted (C), and coronal FLAIR (D) and T1-weighted (E) MRI images before anti-hypertensive therapy. Axial FLAIR image shows abnormal hyperintense signals indicating edema in periventricular and deep white matter and basal ganglia, more so, on right side (arrow) (B). Cerebral edema is observed as hyperintense signal on T2-weighted image in bilateral caudate and lentiform nuclei (black arrow) (C). Coronal FLAIR image shows hyperintense signal changes in dentate nuclei (arrows) (D). Also T2-weighted MRI shows two hyperintense lesions with peripheral hemosiderin rim; chronic hematoma is hypointense on T1-weighted images and hyperintense on T2-weighted images in right external capsule (white arrow), subacute hematoma in right globus pallidus is hyperintense on T1 and T2-weighted images (arrowhead) (E). FLAIR = fluid attenuated inversion recovery F-H. On tenth day of anti-hypertensive therapy; axial FLAIR image (F) demonstrates remarkable regression of high signal intensities in periventricular and deep white matter, axial T2-weighted (G) and coronal FLAIR (H) images show complete losses of high signal intensities in caudate, lentiform and dentate nuclei due to regressions of vasogenic edema. I. On susceptibility weighted imaging, there are millimetric signal losses in bilateral basal ganglia which are compatible with hemorrhagic foci. These were not seen on conventional MRI. FLAIR = fluid attenuated inversion recovery
Reference
-
1. Yeo H, Roman S. Pheochromocytoma and functional paraganglioma. Curr Opin Oncol. 2005; 17:13–18.2. McKinney AM, Sarikaya B, Gustafson C, Truwit CL. Detection of microhemorrhage in posterior reversible encephalopathy syndrome using susceptibility-weighted imaging. AJNR Am J Neuroradiol. 2012; 33:896–903.3. Singh VP, Singh M, Malhotra M, Kumar A, Agarwal AK. Extra-adrenal phaeochromocytoma-a case report of refractory hypertension. Indian Heart J. 2012; 64:203–205.4. Eclavea A, Gagliardi JA, Jezior J, Burton B, Donahue JP. Phaeochromocytoma with central nervous system manifestations. Australas Radiol. 1997; 41:373–376.5. Beltsevich DG, Kuznetsov NS, Kazaryan AM, Lysenko MA. Pheochromocytoma surgery: epidemiologic peculiarities in children. World J Surg. 2004; 28:592–596.6. Kang E, Jeon SJ, Choi SS. Uremic encephalopathy with atypical magnetic resonance features on diffusion-weighted images. Korean J Radiol. 2012; 13:808–811.7. McKinney AM, Short J, Truwit CL, McKinney ZJ, Kozak OS, SantaCruz KS, et al. Posterior reversible encephalopathy syndrome: incidence of atypical regions of involvement and imaging findings. AJR Am J Roentgenol. 2007; 189:904–912.8. Choi JM, Kim YH, Roh SY. Acute hepatic encephalopathy presenting as cortical laminar necrosis: case report. Korean J Radiol. 2013; 14:324–328.9. Camara-Lemarroy CR, Lara-Campos JG, Perez-Contreras E, Rodríguez-Gutiérrez R, Galarza-Delgado DA. Takayasu's arteritis and posterior reversible encephalopathy syndrome: a case-based review. Clin Rheumatol. 2013; 32:409–415.10. Jones BV, Egelhoff JC, Patterson RJ. Hypertensive encephalopathy in children. AJNR Am J Neuroradiol. 1997; 18:101–106.11. Casey SO, Sampaio RC, Michel E, Truwit CL. Posterior reversible encephalopathy syndrome: utility of fluid-attenuated inversion recovery MR imaging in the detection of cortical and subcortical lesions. AJNR Am J Neuroradiol. 2000; 21:1199–1206.12. Chester EM, Agamanolis DP, Banker BQ, Victor M. Hypertensive encephalopathy: a clinicopathologic study of 20 cases. Neurology. 1978; 28(9 Pt 1):928–939.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A case of Posterior Reversible Encephalopathy Syndrome Presenting as Generalized Seizure after Delivery
- Hypertension-induced Posterior Reversible Encephalopathy Syndrome
- Hypertensive Brainstem Encephalopathy Combined with Acute Ischemic Stroke
- A Case of Reversible Posterior Leukoencephalopathy Involving in the Spinal Cord with Pheochromocytoma
- Posterior Reversible Encephalopathy Syndrome in a Patient with Intoxication of Arisaema amurense
