Hypertensive Heart Failure Associated with Middle Aortic Syndrome Reversed Dramatically by Endovascular Management
- Affiliations
-
- 1Division of Cardiology, Department of Internal Medicine, Kyung Hee University Medical Center, Seoul, Korea.
- 2Division of Cardiology, Department of Internal Medicine, Gwangju Veterans Hospital, Gwangju, Korea. kvhwkim@chol.com
- KMID: 1980369
- DOI: http://doi.org/10.4250/jcu.2011.19.3.144
Abstract
- A 42-year-old male patient presented with refractory hypertension and congestive heart failure. He had taken hydrochlorthiazide 50 mg, carvedilol 25 mg, diltiazem 180 mg, and losartan 100 mg per day. Aortogram revealed a severe luminal narrowing in the distal thoracic aorta with a peak systolic pressure gradient of 60 mmHg across the lesion. Endovascular management was performed with 22 x 80 mm self-expandable Nitinol-S stent after predilation with 10 x 40 mm balloon. After endovascular management, the patient's blood pressure, left ventricular ejection fraction (LVEF) and dilated LV dimension were remarkably improved.
Keyword
MeSH Terms
Figure
-
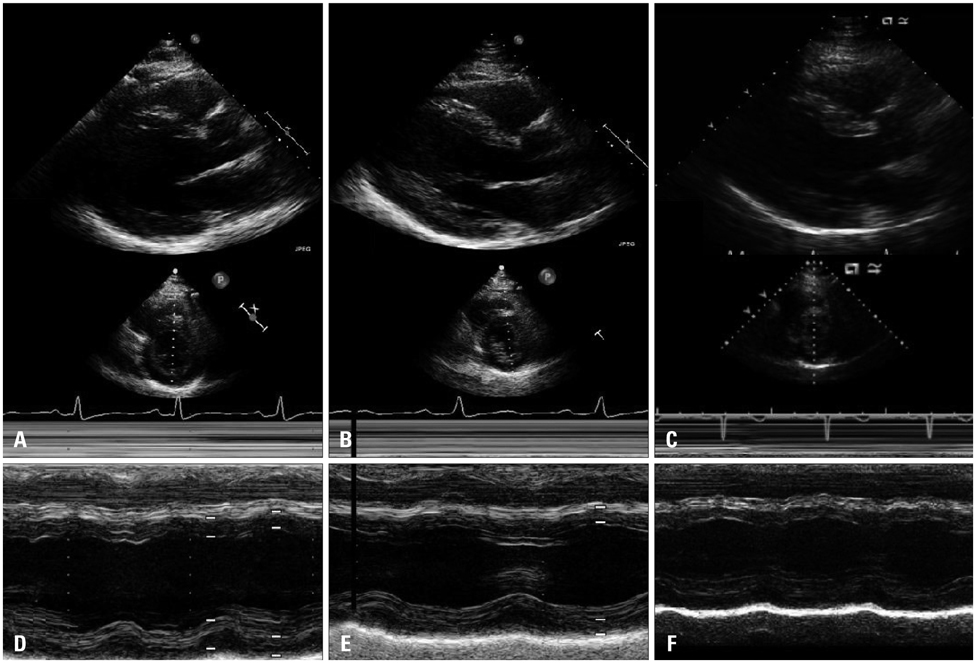
Fig. 1 2-D and M-mode echocardiography before stenting showed a decreased left ventricular ejection fraction and dilated left ventricular dimension (LV end-diastolic dimension was 63 mm) (A and D). In 2 month (B and E) and 6 month follow-up 2-D and M-mode echocardiography after stenting (C and F), the left ventricular ejection fraction and dimension were remarkably improved dimension (LV end-diastolic dimension was 60 mm, 55 mm respectively). LV: left ventricular.
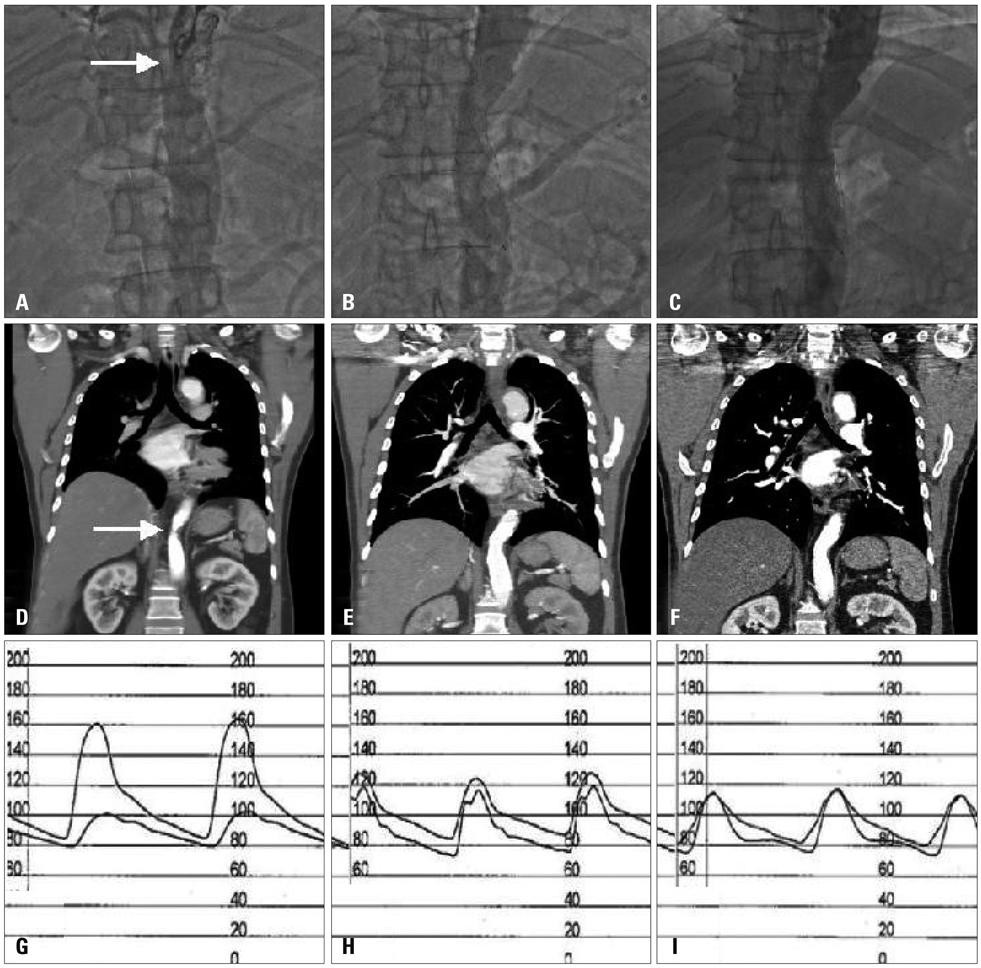
Fig. 2 Aortogram before stenting revealed significant luminal narrowing (arrow) at distal thoracic aorta (A), and after stenting (B) and 6 months follow-up after stenting (C) revealed remarkable improvement of luminal narrowing in the distal thoracic aorta. A chest computed tomography (CT) scan revealed coarctation (arrow) of the descending thoracic aorta (D). Chest CT scan after stenting (E) and 6 months follow-up chest CT scan after stenting (F) showed good apposition of the stent in the thoracic coarctation aorta. The peak pressure gradient across the stenotic lesion revealed 60 mmHg before stenting (G), it was decreased to 8 mmHg (H) after stenting and it was decreased to 0 mmHg 6 months after stenting (I).
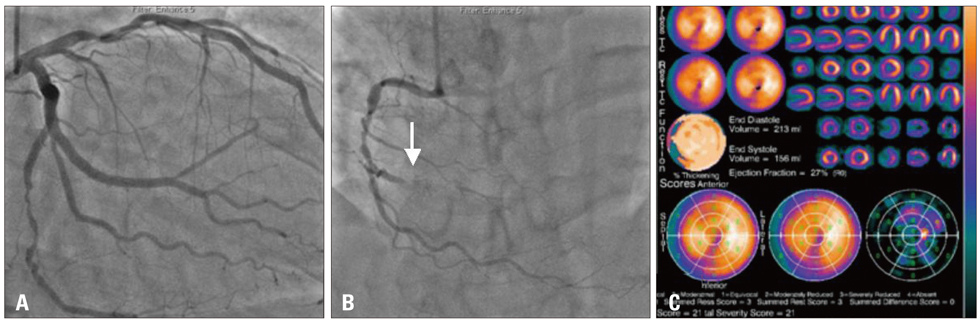
Fig. 3 In coronary angiogram, there was a significant stenosis in the proximal left coronary artery, the middle left circumflex artery and chronic total occlusion (arrow) in the distal right coronary artery. (A and B) A stress test with 99 mTc-tetrofosmin gated myocardial perfusion scintigraphy was performed to evaluate myocardial viability and showed a normal perfusion with global hypokinesia (C).
Reference
-
1. Harrison DA, McLaughlin PR, Lazzam C, Connelly M, Benson LN. Endovascular stents in the management of coarctation of the aorta in the adolescent and adult: one year follow up. Heart. 2001. 85:561–566.
Article2. Mahadevan V, Mullen MJ. Endovascular management of aortic coarctation. Int J Cardiol. 2004. 97:Suppl 1. 75–78.
Article3. Bergamini TM, Bernard JD, Mavroudis C, Backer CL, Muster AJ, Richardson JD. Coarctation of the abdominal aorta. Ann Vasc Surg. 1995. 9:352–356.
Article4. Fuster V, Alexander RW, O'Rourke RA. Hurst's the heart. 2001. 10th ed. New York: McGraw Hill;2390.5. Kim W, Jeong MH, Shim WH, Ahn YK, Kang JC. A successful stenting of the coarctation of aorta in a patient presented with acute pulmonary edema. Int J Cardiol. 2006. 113:267–269.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Periodic Surveillance and Medical Management of Thoracic Aortic Aneurysm
- The Complications and Their Management after Endovascular Aneurysm Repair for the Treatment of Abdominal Aortic Aneurysms
- Anesthetic Management of Endovascular Stent Graft Placement for Thoracic Aortic Diseases: A case report
- Retrograde Aortic Dissection after Thoracic Endovascular Aortic Repair for Descending Aorta: 2 case reports
- Ruptured Abdominal Aortic Aneurysm with Antecedent Endovascular Repair of Abdominal Aortic Aneurysm
