Full mouth rehabilitation on a bilateral condylar fractured patient using orthognathic surgery and dental implant
- Affiliations
-
- 1Divison of Prosthodontics, Department of Dentistry, College of Medicine, University of Ulsan, Asan Medical Center, Seoul, Korea. chahyunsuk@hanmail.net
- 2Division of Oral and Maxillofacial Surgery, Department of Dentistry, College of Medicine, University of Ulsan, Asan Medical Center, Seoul, Korea.
- KMID: 1975116
- DOI: http://doi.org/10.4047/jap.2011.3.1.51
Abstract
- BACKGROUND
Mandibular displacement is a common complication of condylar fracture. In the mandibular displacement due to condylar fracture, it is difficult to restore both esthetics and function without using orthognathic surgery. CASE DESCRIPTION: This clinical report described a full mouth rehabilitation in the patient with bilateral condylar fractures and displaced mandible using bilateral sagittal split ramus osteotomy (BSSRO) and simultaneous dental implant surgery. Mandibular position was determined by model surgery through the diagnostic wax up and restoration of fractured teeth. The precise amount of the mandibular shift can be obtained from the ideal intercuspation of remaining teeth. CLINICAL IMPLICATION: Mandibular displacement by both condylar fractures can be successfully treated by orthognathic surgery. Determination of occlusal plane and visualization from diagnostic wax up are mandatory for mandibular repositioning of model surgery. Stable occlusion and regular recall check up are needed for long-term outcome.
MeSH Terms
Figure
-
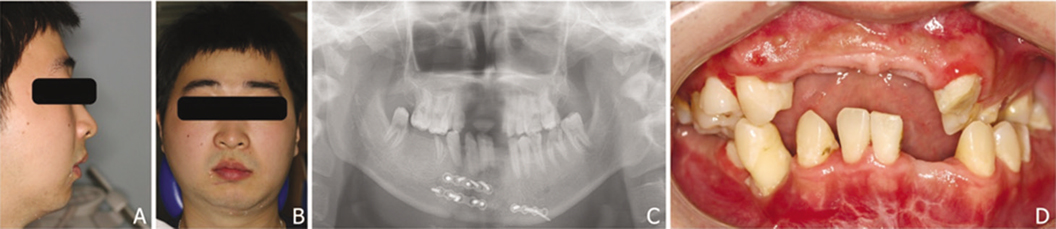
Fig. 1 Initial facial photos and radiograph. A: Lateral facial profile, B: Frontal facial profile, C: Panoramic radiograph, D: Intraoral frontal view.

Fig. 2 Facebow transfer A and diagnostic model mounted on a semi-adjustable articulator B.
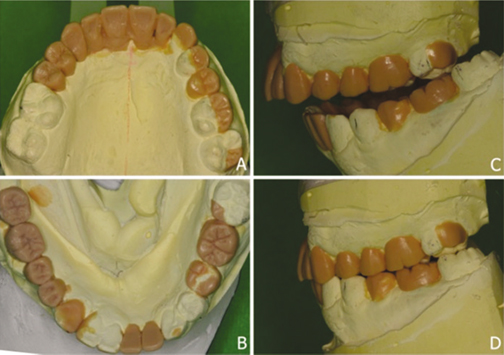
Fig. 3 Diagnostic wax up and model surgery. A: Occlusal view of Maxilla, B: Occlusal view of Mandible, C: Initial status of mounted model, D: Remounting of lower cast to simulate BSSRO.

Fig. 4 Initial overbite and overjet relationship with try in of final metal-ceramic crown.

Fig. 5 Panoramic radiograph after implant and BSSRO surgery.

Fig. 6 A: Panoramic radiograph after one year later from delivery of prosthesis, B: Frontal view of definitive fixed prosthesis at one year recall check up.
Reference
-
1. Kazanjian VH, Converse JH. The surgical treatment of facial injuries. 1974. 3rd ed. Baltimore: Williams & Wilkins.2. Spitzer WJ, Vanderborght G, Dumbach J. Surgical management of mandibular malposition after malunited condylar fractures in adults. J Craniomaxillofac Surg. 1997. 25:91–96.3. Hinds EC, Parnes EI. Late management of condylar fractures by means of subcondylar osteotomy: reports of cases. J Oral Surg. 1966. 24:54–59.4. Harper R, Weinberg S. Treatment of malunited, unusually displaced bilateral condylar fractures: report of case. J Oral Surg. 1978. 36:716–719.5. Rubens BC, Stoelinga PJ, Weaver TJ, Blijdorp PA. Management of malunited mandibular condylar fractures. Int J Oral Maxillofac Surg. 1990. 19:22–25.6. Türp JC, Stoll P, Schlotthauer U, Vach W, Strub JR. Computerized axiographic evaluation of condylar movements in cases with fractures of the condylar process: a follow up over 19 years. J Craniomaxillofac Surg. 1996. 24:46–52.7. Becking AG, Zijderveld SA, Tuinzing DB. Management of posttraumatic malocclusion caused by condylar process fractures. J Oral Maxillofac Surg. 1998. 56:1370–1374.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Full-mouth rehabilitation by immediate implantation combined with orthognathic surgery: a clinical report
- Application of ARCUS digma I, II systems for full mouth reconstruction: a case report
- Full mouth rehabilitation of a patient using monolithic zirconia and dental CAD/CAM system: a case report
- Full mouth fixed implant rehabilitation in a patient with generalized aggressive periodontitis
- Ten-year follow-up of full mouth rehabilitation with fixed prostheses using implants and natural tooth
