Endocrinol Metab.
2012 Dec;27(4):334-339. 10.3803/EnM.2012.27.4.334.
A Case of Multiple Osteoporotic Compression Fractures in Young Man with Budd-Chiari Syndrome
- Affiliations
-
- 1Division of Endocrinology and Metabolism, Department of Internal Medicine, Korea University College of Medicine, Seoul, Korea. kahlua99@hanmail.net
- KMID: 1973800
- DOI: http://doi.org/10.3803/EnM.2012.27.4.334
Abstract
- Osteoporosis in young men is extremely rare. In this report, we demonstrate a rare case of multiple vertebral fractures discovered in a young man with Budd-Chiari syndrome without prior history of trauma. A 29-year-old man was diagnosed as Budd-Chiari syndrome 12 years ago and underwent a mesocaval shunt to relieve the hepatic vein obstruction and was on warfarin therapy. He suffered from low back pain and it was not relieved by analgesics. A T-L spine X-ray revealed multiple compression fractures and the z-score at lumbar spine was -3.7 which is below the expected range for that age. The patient was treated with calcium, vitamin D and bisphosphonate, and showed clinical improvement. This case highlights the importance of the investigation for secondary osteoporosis in young adults with an underlying disease that alters bone metabolism.
Keyword
MeSH Terms
Figure
-
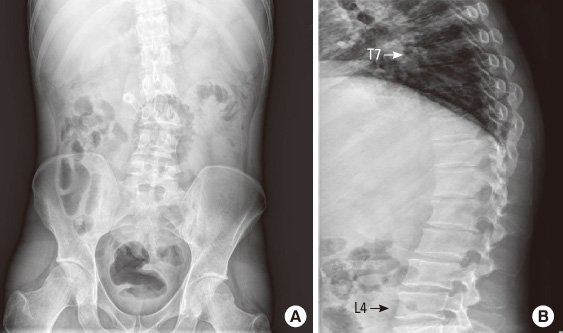
Fig. 1 The simple X-ray images of the patient. (A) Abdominal plain film shows mild scoliosis and stent of mesocaval shunt. (B) Lateral plain film shows multiple compression fractures at T7 through L4.

Fig. 2 Computed tomography image of T-L spine shows multiple compression fractures at T7 to L5 spine.

Fig. 3 Bone scan shows hot uptake at right 4th, 10th ribs and left 2nd, 5th, and 8th ribs. Diffuse hot uptake at T7 to L5 vertebrae is also noted.
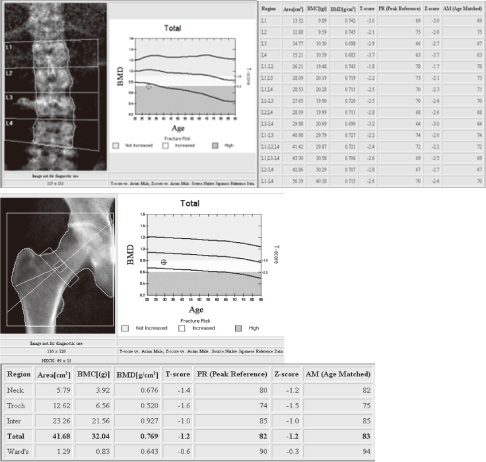
Fig. 4 Bone densitometry demonstrates low bone mineral density at lumbar spine and right femur.
Reference
-
1. Chung HY. Osteoporosis diagnosis and treatment 2007. J Korean Endocr Soc. 2008. 23:76–108.2. Hofbauer LC, Hamann C, Ebeling PR. Approach to the patient with secondary osteoporosis. Eur J Endocrinol. 2010. 162:1009–1020.3. Khosla S, Lufkin EG, Hodgson SF, Fitzpatrick LA, Melton LJ 3rd. Epidemiology and clinical features of osteoporosis in young individuals. Bone. 1994. 15:551–555.4. Ferrari S, Bianchi ML, Eisman JA, Foldes AJ, Adami S, Wahl DA, Stepan JJ, de Vernejoul MC, Kaufman JM. For the IOF Committee of Scientific Advisors Working Group on Osteoporosis Pathophysiology. Osteoporosis in young adults: pathophysiology, diagnosis, and management. Osteoporos Int. 2012. 23:2735–2748.5. López-Larramona G, Lucendo AJ, González-Castillo S, Tenias JM. Hepatic osteodystrophy: an important matter for consideration in chronic liver disease. World J Hepatol. 2011. 3:300–307.6. Valla DC. Primary Budd-Chiari syndrome. J Hepatol. 2009. 50:195–203.7. Goral V, Simsek M, Mete N. Hepatic osteodystrophy and liver cirrhosis. World J Gastroenterol. 2010. 16:1639–1643.8. Moschen AR, Kaser A, Stadlmann S, Millonig G, Kaser S, Muhllechner P, Habior A, Graziadei I, Vogel W, Tilg H. The RANKL/OPG system and bone mineral density in patients with chronic liver disease. J Hepatol. 2005. 43:973–983.9. Szalay F, Hegedus D, Lakatos PL, Tornai I, Bajnok E, Dunkel K, Lakatos P. High serum osteoprotegerin and low RANKL in primary biliary cirrhosis. J Hepatol. 2003. 38:395–400.10. Pereira FA, Facincani I, Jorgetti V, Ramalho LN, Volpon JB, Dos Reis LM, de Paula FJ. Etiopathogenesis of hepatic osteodystrophy in Wistar rats with cholestatic liver disease. Calcif Tissue Int. 2009. 85:75–83.11. Janes CH, Dickson ER, Okazaki R, Bonde S, McDonagh AF, Riggs BL. Role of hyperbilirubinemia in the impairment of osteoblast proliferation associated with cholestatic jaundice. J Clin Invest. 1995. 95:2581–2586.12. Collier JD, Ninkovic M, Compston JE. Guidelines on the management of osteoporosis associated with chronic liver disease. Gut. 2002. 50:Suppl 1. i1–i9.13. Arteh J, Narra S, Nair S. Prevalence of vitamin D deficiency in chronic liver disease. Dig Dis Sci. 2010. 55:2624–2628.14. Holick MF, Binkley NC, Bischoff-Ferrari HA, Gordon CM, Hanley DA, Heaney RP, Murad MH, Weaver CM. Endocrine Society. Evaluation, treatment, and prevention of vitamin D deficiency: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2011. 96:1911–1930.15. Hamada T, Fondevila C, Busuttil RW, Coito AJ. Metalloproteinase-9 deficiency protects against hepatic ischemia/reperfusion injury. Hepatology. 2008. 47:186–198.16. Rezaieyazdi Z, Falsoleiman H, Khajehdaluee M, Saghafi M, Mokhtari-Amirmajdi E. Reduced bone density in patients on long-term warfarin. Int J Rheum Dis. 2009. 12:130–135.17. Watts NB, Adler RA, Bilezikian JP, Drake MT, Eastell R, Orwoll ES, Finkelstein JS. Endocrine Society. Osteoporosis in men: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2012. 97:1802–1822.18. Collier J. Bone disorders in chronic liver disease. Hepatology. 2007. 46:1271–1278.19. Ebeling PR. Clinical practice. Osteoporosis in men. N Engl J Med. 2008. 358:1474–1482.20. Wang C, Nieschlag E, Swerdloff R, Behre HM, Hellstrom WJ, Gooren LJ, Kaufman JM, Legros JJ, Lunenfeld B, Morales A, Morley JE, Schulman C, Thompson IM, Weidner W, Wu FC. Investigation, treatment and monitoring of late-onset hypogonadism in males: ISA, ISSAM, EAU, EAA and ASA recommendations. Eur J Endocrinol. 2008. 159:507–514.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Budd-Chiari Syndrome with IVC Web Treated by Balloon Dilatation
- Budd-Chiari syndrome associated with diaphragmatic hernia: A case report
- Hepatoblastoma with budd-chiari syndrome in child: a case report
- Stasis Dermatitis Associated with Budd-Chiari Syndrome
- A Case of Budd Chiari Syndrome Caused by Membraneous Obstruction of Suprahepatic Inferior Vena Cava
