Adenocarcinoma Surrounding Emphysema Mimicking Cavitary Pneumonia
- Affiliations
-
- 1Department of Respiratory and Critical Care Medicine, College of Medicine, Kyung Hee University, Seoul, Korea. honglung@chol.com, medgrant@hanmail.net
- 2Department of Thoracic and Cardiovascular Surgery, College of Medicine, Kyung Hee University, Seoul, Korea.
- 3Department of Pathology, College of Medicine, Kyung Hee University, Seoul, Korea.
- KMID: 1910101
- DOI: http://doi.org/10.4046/trd.2007.63.2.200
Abstract
- Adenocarcinoma presenting as a solitary mass with a cavity in chest computed tomogram is rare. A few reports have suggested an association between lung cancer and emphysema. We report a case of adenocarcinoma surrounding pulmonary emphysema that mimicked fungal pneumonia. This case highlights the need for cliniclians to be aware of the potential development of lung cancer in patients with emphysema.
Keyword
Figure
-
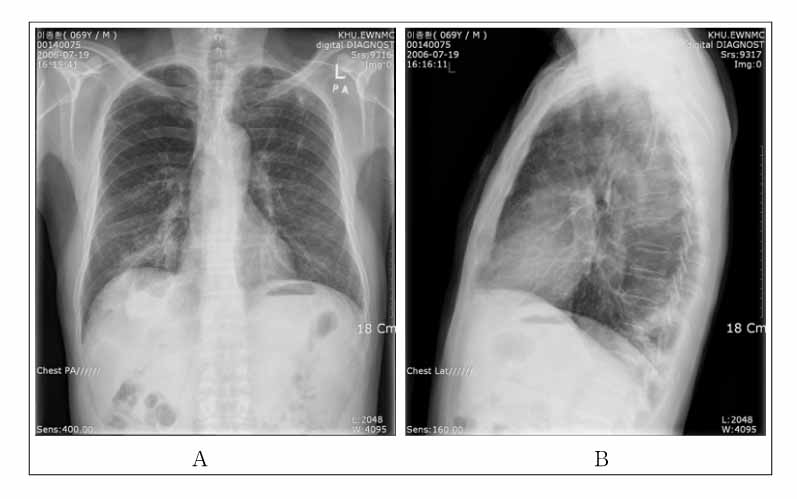
Figure 1 X-ray shows airspace consolidation on both lower lobe and a large cavity in the right lower lobe underlying emphysema and inactive tuberculosis on the left upper lobe (A: Chest PA view, B: Chest Right lateral view).

Figure 2 Chest computed tomography shows a mass surrounding a pulmonary cavity with septae in the right lower lobe.
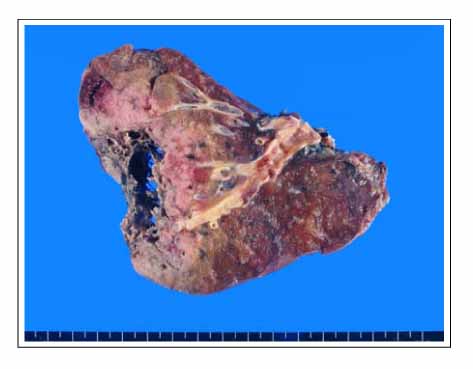
Figure 3 Gross finding shows ill defined, gray-white to yellow-tan mass with central septated cavitary lesion, measuring 9×8.5×4.5 cm at right lower lobe of lung. There are emphysematous changes in superior segment and lateral basal segment (not shown).
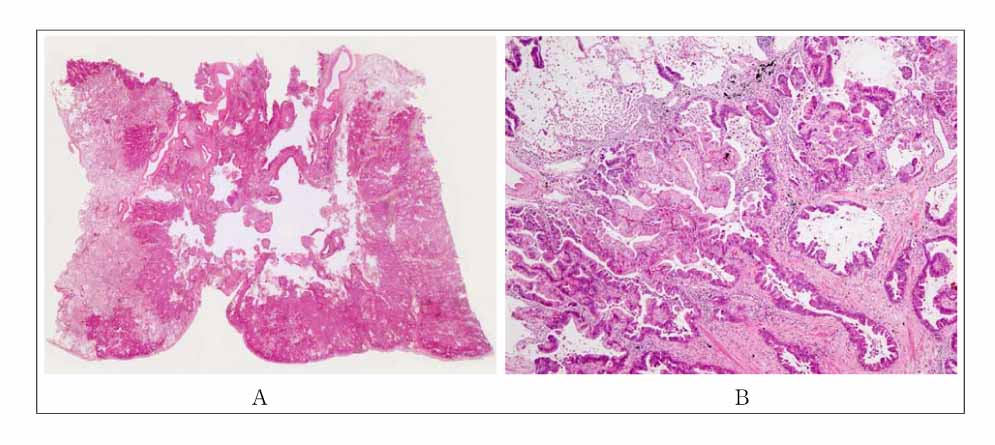
Figure 4 A. On lower power field, infiltrating tumor tissue around central septated cavitary lesion, indicating emphysema is seen. There are surrounding satellite nodules and pleural dimpling. B. Microspcopic finding shows moderately differentiated adenocarcinoma. (A: H&E, ×1, B: H&E, ×200)
Reference
-
1. Greco RJ, Steiner RM, Goldman S, Cotler H, Patchefsky A, Cohn HE. Bronchioloalveolar cell carcinoma of the lung. Ann Thorac Surg. 1986. 41:652–656.2. Dinkel E, Mundinger A, Schopp D, Grosser G, Hauenstein KH. Diagnostic image in metastatic lung disease. Lung. 1990. 168:S1129–S1136.3. Dodd GD, Boyle JJ. Excavating pulmonary metastases. Am J Roentgenol Radium Ther Nucl Med. 1961. 85:277–293.4. Watts MA, Klayton RJ, Munzel TL. Bullous emphysema and carcinoma of the lung: case report. Mil Med. 1982. 147:320. 323.5. Goldstein MJ, Snider GL, Liberson M, Poske RM. Bronchogenic carcinoma and giant bullous disease. Am Rev Respir Dis. 1968. 97:1062–1070.6. Stoloff IL, Kanofsky P, Magilner L. The risk of lung cancer in males with bullous disease of the lung. Arch Environ Health. 1971. 22:163–167.7. Ogawa D, Shiota Y, Marukawa M, Hiyama J, Mashiba H, Yunoki K, et al. Lung cancer associated with pulmonary bulla. case report and review of literature. Respiration. 1999. 66:555–558.8. Freant LJ, Joseph WL, Adkins PC. Scar carcinoma of the lung. Fact or Fantasy? Ann Thorac Surg. 1974. 17:531–537.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Clinical Investigation of Cavitary Tuberculosis and Tuberculous Pneumonia
- Subcutaneous Emphysema Mimicking Gas Gangrene Following Perforation of the Rectum: A Case Report
- A Case of Measles Pneumonia Complicated by Subcutaneous Emphysema and Pneumomediastinum in an 18-year-old Patient
- A Case of Nonspecific Interstitial Pneumonia Complicated with Spontaneous Pneumomediastinum, Subcutaneous Emphysema and Pneumatosis Interstinalis
- A Cavitary Lesion Changed to Pulmonary Nodule
