A Comparison of Fusion Rates and Clinical Results Between Single-Level Cervical Corpectomy and Two-Level Discectomies and Fusion with Plating
- Affiliations
-
- 1Department of Orthopaedic Surgery, Kangdong Sacred Heart Hospital, College of Medicine, Hallym University, Seoul, Korea. skw@hallym.or.kr
- KMID: 1897088
- DOI: http://doi.org/10.4184/jkss.2002.9.1.35
Abstract
-
STUDY DESIGN: A retrospective study.
OBJECTIVES
To compare the radiographic and clinical results of two-level discectomies and fusion with plating and a singlelevel corpectomy with plating. SUMMARY OF LITERATURE REVIEW: Previous studies of multisegment fusion have shown decreased fusion rates correlating with the number of increasing levels, and the use of anterior plate in multilevel fusions may be warranted because of the increased pseudoarthrosis rates.
MATERIALS AND METHODS
A total 30 consecutive patients operated at our institutions between Oct. 1995 and Mar. 2000 were entered into this study. Twenty patients with cervical spondylosis had performed two-level discectomies with tricortical bone grafts and plating, and ten patients with cervical myelopathy had a single-level corpectomy with plating. Follow up averaged 2.4 years, radiographic and clinical follow up evaluation was performed. We assessed the radiologic value by postoperative and follow-up sagittal radiograms at monthly intervals until fusion was judged to be solid, and the clinical evaluation by Odom's criteria.
RESULTS
Comparing the radiographic data between the two groups of patients, the values were not different. Of the thirty patients, no non-unions occurred in all patients. The average amount of graft collapse for patients with single-level corpectomy with plating or a two-level discectomy with plating was less than 1 mm for both groups. And, the average amount of kyphotic deformity was less than 1 degrees for both groups. The clinical results of the operations graded by Odom's criteria are no statistical significance between the two groups. (p < 0.9, chi test)
CONCLUSION
There is no significant statistical differences for two-level discectomies with plating and a single-level corpectomy with plating in fusion rate and clinical results, and each methods can be used a viable alternative procedure by anatomical structure that were primarily causing the neural impingement with more reliable fusion rates.
Keyword
MeSH Terms
Figure
-
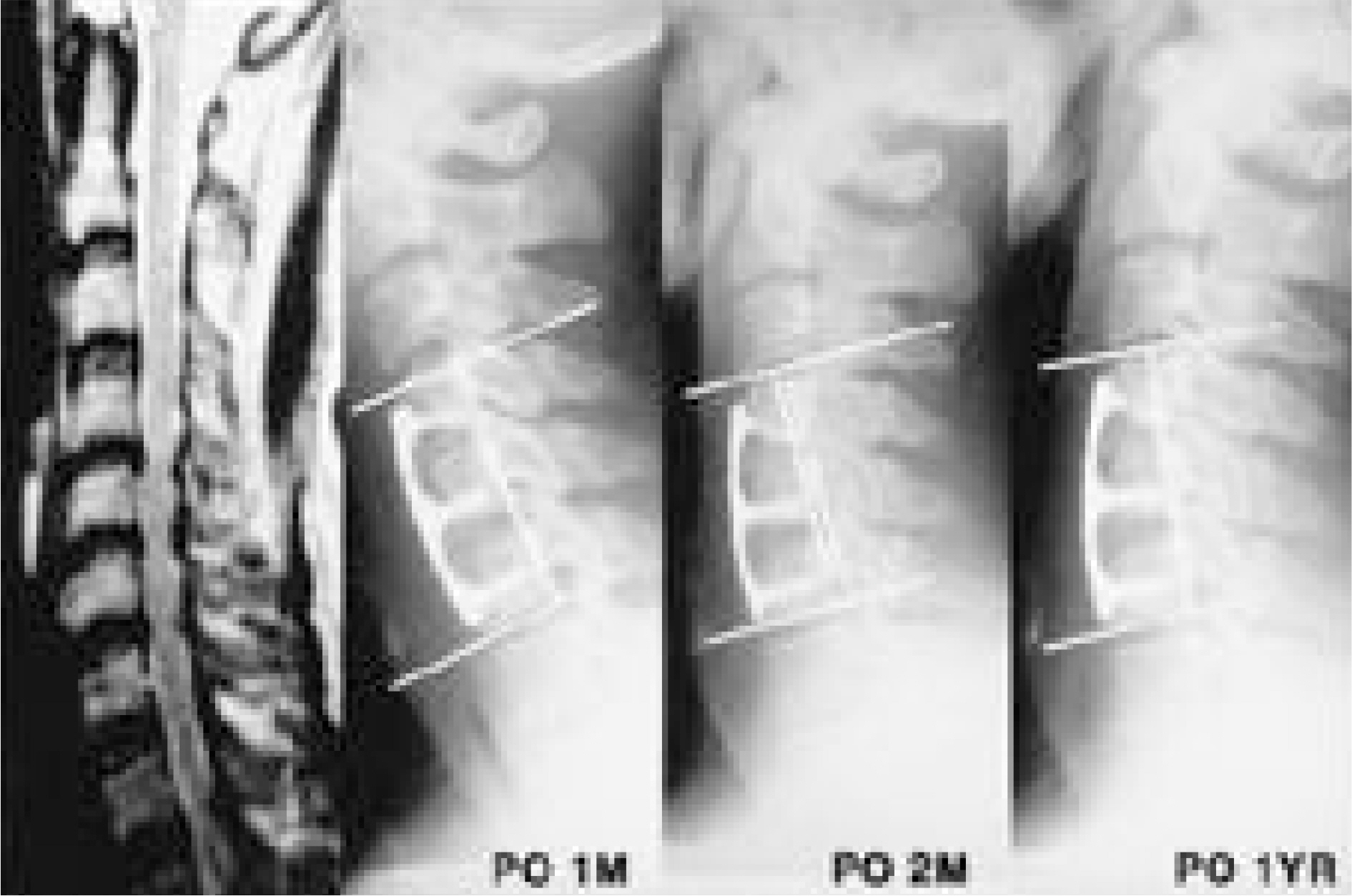
Fig. 1. Preoperative lateral radiography of 57 years old man shows disc degeneration of C4-5, C5-6 and segmental instability at the level of C4-5, C5-6 in flexion-extension views. MRI shows posterior epidural mass at C4-5 and C5-6 disc level on T2-weighted sagittal image. Postoperative 1 month followup lateral radiography shows no change of lordotic curve after two level discectomy and fusion with plating. Postoperative 2 month followup lateral radiography shows breakage of screws on C4 vertebral body and loss of cervical lordosis by 5°. Postoperative 1 year followup lateral radiography shows maintenance of kyphotic angle and solid fusion of graft bone.

Fig. 2-A. Preoperative lateral radiography of 46 years old woman shows cervical kyphotic angle by 20° and anterior subluxation of C4 on C5. Fig. 1-B. Postoperatively lateral radiography with C5 corpectomy and C4-6 anterior interbody fusion with tricortical bone graft and plate shows increased cervical lordosis angle by 5°. Postoperative 1.5 year followup lateral radiography shows no loss of cervical lordotic curve.

Fig. 3-A. Preoperative lateral radiography with 46 years old man shows narrowed disc space and calcification along the posterior longitudinal ligament from the upper portion of C4 to lower portion of C6. Also the abnormal ossification was shown in sagittal and axial CT scan. Fig. 1-B. Postoperative 1, 3, 6 month followup radiographies with C5 corpectomy and C4-6 anterior interbody fusion with tricortical bone graft and plate show cervical lordotic angle by 20°and no evidence of graft collapse.
Reference
-
1). Bohlman HH. Cervical spondylosis with moderate to severe myelopathy: A report of seventeen cases treated by Robinson anterior cervical discectomy and fusion. Spine. 2:151–6. 1977.2). Bohlman HH. Cervical spondylosis and myelopathy. Instr Course Lect Am Acad Orthop Surg. 44:81–97. 1995.3). Bohlman HH, Emery SE, Goodfellow DB. Robinson anterior cervical discectomy and arthrodesis for cervical radiculopathy. Instr Course Lect Am Acad Orthop Surg. 75:1298–307. 1993.4). Capen D, Rah A, Nagelberg S. Clinical significance of instrumented vuersus non instrumented anterior cervical discectomy and fusion. Presented at the annual meeting of the North American Spine Society, New York, NY, October 25. 1997.5). Connolly PJ, Esses SI, Kostuik JP. Anterior cervical fusion: Outcome analysis of patients fused with and without anterior cervical plates. J Spinal Disord. 9:202–6. 1996.6). Coric D, Branch CL Jr, Jenkins JD. Revision of anterior cervical pseudarthrosis with anterior allograft fusion and plating. J Neurosurg. 86:969–74. 1997.
Article7). Emery SE, Bolesta MJ, Banks MA. Robinson anterior cervical fusion. Comparison of standard and modified techniques. Spine. 19:660–3. 1994.8). Eery SE, Fisher JRS, Bohlman HH. Higher inci -dence of pseudarthrodesis and poor outcomes for three-level anterior cervical discectomy and fusion. Presented at the annual meeting or the Cervical Spine Research Society, Palm Becah, FL, December 6. 1996.9). Griffith SL, Zogbi SW, Guyer RD. Biochemic al comparison of anterior instrumentation for the cervical spine. J Spinal Disord. 8:429–38. 1995.10). Odom GL, Finney W, Woodhall B. Cervical disc lesions. JAMA. 166:23–8. 1958.11). Phillips FM, Carlsion GC, Emery SE. Anterior cervical pseudarthrosis. Natural history and treatment. Spine. 22:1585–9. 1997.12). Robinson RA, Walker AE, Ferlic DC. T he results of anterior interbody fusion of the cervical spine. J Bone Joint Surg [Am]. 44:1569–87. 1962.13). Shapiro SA, Snyder W. S pinal instrumentation with a low complication rate. Surg Neurol. 48:466–74. 1997.14). Shapiro S. Banked fibula and the looking anterior cervical plate in anterior cervical fusions following cervical discectomy. J Neurosurg. 84:161–5. 1996.15). Swank ML, Lowery GL, Bhat AL. Anterior cervical allograft arthrodesis and instrumentation: multilevel interbody grafting or strut graft reconstruction. Eur Spine J. 6:138–43. 1997.
Article16). Vaccaro AR, Balderston RA. Anterior plate instrumentation for disorders of the subaxial cervical spine. Clin Orthop. 335:112–21. 1997.
Article17). Wang JC, McDonough PW, Kanim LEA. Single-level anterior cervical discectomy and fusion: Plate vs no plate. J Spinal Disord. 12:467–71. 1999.18). Wang JC, Mcdough PW, Endow KK. Increased fusion rates with cervical plating for two-level anterior cervical discectomy and fusion. Spine. 25:41–5. 2000.
Article19). Zoega B, Lind B, Rosen H. Outcome after anterior cervical fusion with or without plate fixation. Presented at the annual meeting of the North American Spine Society, New York, NY, October 25. 1997.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Analysis of Noninstrumented Anterior Cervical Discectomy and Interbody Fusion in Degenerative Cervical Disease
- A Comparison of Clinical and Radiological Outcome Between Two-Level Discectomy and One-Level Corpectomy for Cervical Degenerative Disc Disease
- Expandable Cage for Cervical Spine Reconstruction
- A Comparison of Corpectomy and Bisegmental Diskectomy in Anterior Cervical Fusion
- Comparisons of Two-level Discectomy and Fusion with Cage Alone versus Single-level Corpectomy and Fusion with Plate in the Treatment of Cervical Degenerative Disc Disease
