Tuberc Respir Dis.
2007 Jul;63(1):78-82. 10.4046/trd.2007.63.1.78.
Two Cases of Benign Solitary Schwannoma with Pleural Effusion
- Affiliations
-
- 1Department of Internal Medicine, Pusan National University College of Medicine, Busan, Korea. leemk@pusan.ac.kr
- 2Diagnostic Radiology, Pusan National University College of Medicine, Busan, Korea.
- 3Thoracic Surgery, Pusan National University College of Medicine, Busan, Korea.
- KMID: 1877321
- DOI: http://doi.org/10.4046/trd.2007.63.1.78
Abstract
- Schwannoma represents approximately 40% of neurogenic tumors arising in the mediastinum, and develops along the sympathetic or parasympathetic chain, intercostals nerve, and spinal ganglia. It is usually asymptomatic, and is confronted accidentally but can produce chest pain, cough and dyspnea. However, dyspnea with pleural effusion is rare in patients with benign schwannoma. We encountered two cases of benign schwannoma with pleural effusion. Both cases had similar initial symptoms and the characteristics of a mass but the characteristics of pleural effusion analysis were different. The benign schwannoma was confirmed in two cases using VATS (video-assisted tharawswpic surgery).
Keyword
MeSH Terms
Figure
-
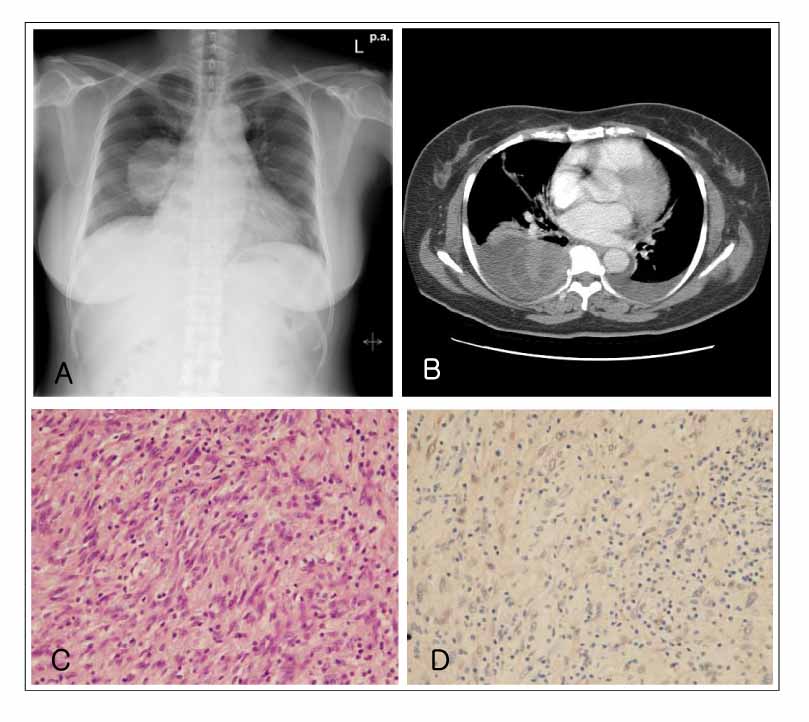
Figure 1 (A) Posteroanterior chest radiograph shows large mass on right lower lung field. (B) Computed tomography shows bilateral pleural effusion and round-ovoid shaped mass on right paravertebral area. (C) Photomicrograph of the specimen. Palisading appearance of spindle cells are seen (H&E stain, ×100). (D) Tumor cells are uniformly reactive for S-100 (S-100 stain, ×100).
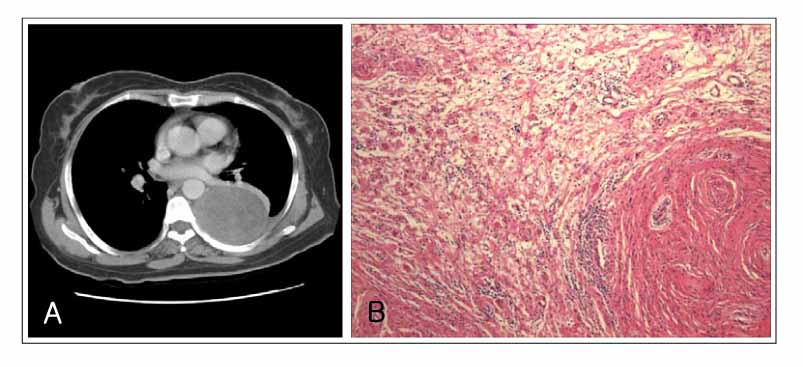
Figure 2 (A) Chest CT scan after drainage shows rounded huge mass in left paravertebral region. (B) Photomicrograph of the specimen. Schwannoma showing sharp partitioning of tumor into cellular Antoni A and myxoid Antoni B areas. Hypocellular zones have microcystic change and inflammatory cell infiltrations (H&E stain, ×100).
Reference
-
1. Kim H, Yang JM, Chung KC, Kim YH, Kang JH, Chung WS. Spontaneous hemothorax in a patient with posterior mediastinal neurilemmoma: a case report. Korean J Thorac Cardiovasc Surg. 2004. 37:1019–1021.2. Das Gupta TK, Brasfield RD, Strong EW, Hajdu SI. Benign solitary Schwannoma (neurilemomas). Cancer. 1969. 24:355–366.3. Bozkurt AK. Schwannoma as a cause of Pancoast's syndrome. Intern Med J. 2002. 32:108–109.4. Moinuddeen K, Baltzer JW, Zama N. Diaphragmatic eventration: an uncommon presentation of a phrenic nerve schwannoma. Chest. 2001. 119:1615–1616.5. Kim DY, Cho CH, Ahn CM, Sohn HY. A case of benign solitary schwannoma of the chest wall. Korean J Med. 1987. 33:119–123.6. Kwon YS, Koh WJ, Kim HJ, Han JH, Lee KS, Shim YM. Two cases of Endobronchial Neurilemmoma and Review of the Literature in Korea. Tuberc Respir Dis. 2007. 62:129–133.7. Kim HG, Park SJ, Kwon SH, Hong SJ, Lee JS, Lee MS, et al. A case of schwannoma induced stenosis of superior mesenteric artery. Korean J Med. 2004. 66:86–90.8. Tanita T, Ohkuda K, Nitta S, Hashimoto K, Nakada T. A case of intrathoracic neurinoma presenting as hemothorax. Nihon Kyobu Shikkan Gakkai Zasshi. 1981. 19:127–130.9. Lee MH, Graham AN, Nicholson AG, Pastorino U. Solitary cellular schwannoma presenting with haemothorax. J R Soc Med. 1998. 91:596–597.10. Ishibashi H, Akamatsu H, Sunamori M, Komori H, Shirasawa S. A case of giant dumbbell shaped schwannoma with massive pleural effusion. Kyobu Geka. 2001. 54:742–746.11. Janowitz P, Meier F, Reisig J. Gastric schwannoma as a rare differential diagnosis of pleural effusion. Z Gastroenterol. 2002. 40:925–928.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Giant, Benign Schwannoma Associated with Total Lung Collapse by Bloody Effusion
- Diagnostic Value of LDH and its Isoenzyme in Pleural Effusion
- Diagnostic Tools of Pleural Effusion
- The Utility of Pleural Adenosine Deaminase for Diagnosis of Differentiating Tuberculous Pleural Effusion in Children
- Ultrasonographic Localization of Solitary Fibrous Tumor of Pleura: Case Report
