Korean Circ J.
2007 Feb;37(2):87-90. 10.4070/kcj.2007.37.2.87.
Intracoronary Stent Deployment without Antiplatelet Agents in a Patient with Idiopathic Thrombocytopenic Purpura
- Affiliations
-
- 1Division of Cardiology, Department of Internal Medicine, The Catholic University of Korea, Seoul, Korea. kbseung@catholic.ac.kr
- KMID: 1859087
- DOI: http://doi.org/10.4070/kcj.2007.37.2.87
Abstract
- Deciding on the appropriate antiplatelet therapy is a challenge when treating patients with idiopathic thrombocytopenic purpura (ITP) and who are undergoing percutaneous coronary intervention (PCI). We describe here a case of PCI in a patient with chronic, refractory ITP. A 61-year-old woman presented with exertional chest pain and a low platelet count (4 x 109/L) at admission. Coronary angiography revealed 99% stenosis of the mid left anterior descending artery and 95% stenosis of the mid left circumflex artery. Antiplatelet agents couldn't be administered because of the risk of bleeding. After transfusion of platelets and administering intravenous immunoglobulin, we deployed baremetal stents in both lesions without administering any antiplatelet agents. Although focal in-stent restenosis developed 5 months later, there was no episode of stent thrombosis despite not using antiplatelet agents. The present case suggests that the rate of stent thrombosis may be lower was previously thought and antiplatelet therapy may be considered on a case by case for patient suffering with thrombocytopenia.
MeSH Terms
-
Arteries
Chest Pain
Constriction, Pathologic
Coronary Angiography
Female
Hemorrhage
Humans
Immunoglobulins
Middle Aged
Myocardial Infarction
Percutaneous Coronary Intervention
Platelet Aggregation Inhibitors*
Platelet Count
Purpura, Thrombocytopenic, Idiopathic*
Stents*
Thrombocytopenia
Thrombosis
Immunoglobulins
Platelet Aggregation Inhibitors
Figure
-
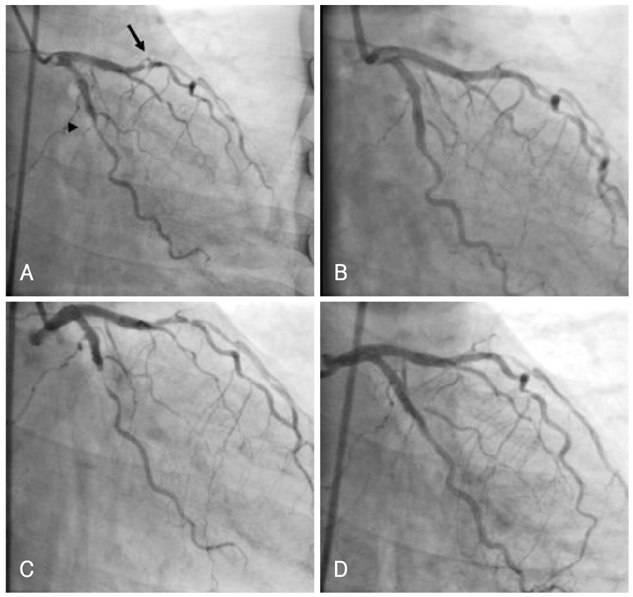
Fig. 1 A case of intracoronary stent playment in a patients with idiopathic thrombocytopenia purpura. A: coronary angiogram in the right anterior oblique view showed 99% stenosis in the middle segment of the left anterior descending artery (arrow) and 95% stenosis in the middle segment of the left circumflex artery (arrow head). B: percutaneous coronary intervention was performed successfully with baremetal stents in both stenotic lesions. C: 5 months later, focal in-stent restenosis developed in both lesions in which the baremetal stents were deployed. D: balloon angioplasty was performed in both in-stent restenotic lesions and mild residual stenotic lesions were left.
Reference
-
1. Cines DB, Blanchette VS. Immune thrombocytopenic purpura. N Engl J Med. 2002. 346:995–1008.2. Leon MB, Baim DS, Popma JJ, et al. A clinical trial comparing three antithrombotic drug regimens after coronary artery stenting. N Engl J Med. 1998. 339:1665–1671.3. Koike R, Suma H, Oku T, Satoh H, Samade Y, Takeuchi A. Combined coronary revascularization and splenectomy. Ann Thorac Surg. 1989. 48:853–854.4. Paolini R, Zamboni S, Ramazzina E, Zampieri P, Cella G. Idiopathic thrombocytopenic purpura treated with steroid therapy does not prevent acute myocardial infarction: a case report. Blood Coagul Fibrinolysis. 1999. 10:439–442.5. Fruchter O, Blich M, Jacob G. Fatal acute myocardial infarction during severe thrombocytopenia in a patient with idiopathic thrombocytopenic purpura. Am J Med Sci. 2002. 323:279–280.6. Hofmeister EP. Coronary artery bypass grafting in chronic immune mediated thrombocytopenic purpura: preoperative treatment with intravenous immunoglobulin and corticosteroids. Mil Med. 1995. 160:624–625.7. Mathew TC, Vasudevan R, Leb L, Pezzella SM, Pezzella AT. Coronary artery bypass grafting in immune thrombocytopenic purpura. Ann Thorac Surg. 1997. 64:1059–1062.8. Crouch ED, Watson LE. Intravenous immunoglobulin-related acute coronary syndrome and coronary angiography in idiopathic thrombocytopenic purpura: a case report and literature review. Angiology. 2002. 53:113–117.9. Paolini R, Fabris F, Cella G. Acute myocardial infarction during treatment with intravenous immunoglobulin for idiopathic thrombocytopenic purpura(ITP). Am J Hematol. 2000. 65:177–178.10. Fischman DL, Leon MB, Baim DS, et al. A randomized comparision of coronary stent placement and balloon angioplasty in the treatment of coronary artery disease. N Engl J Med. 1994. 331:496–501.11. Ong AT, Hoye A, Aoki J, et al. Thirty-day incidence and six-month clinical outcome of thrombotic stent occlusion after bare-metal, sirolimus, or paclitaxel stent implantation. J Am Coll Cardiol. 2005. 45:947–953.12. Park SH, Hong GR, Seo HS, Tahk SJ. Stent thrombosis after successful drug-eluting stent implantation. Korean Circ J. 2005. 35:163–171.13. Choi BR, Lee CW, Park SW. Late stent thrombosis associated with late stent malapposition after drug-eluting stenting: a case report. Korean Circ J. 2006. 36:472–475.14. Iakovou I, Schmidt T, Bonizzoni E, et al. Incidence, predictors, and outcomes of thrombosis after successful implantation of drug-eluting stents. JAMA. 2005. 293:2126–2130.15. Caputo RP, Abraham S, Churchill D. Transradial coronary stent placement in a patient with severe idiopathic autoimmune thrombocytopenic purpura. J Invasive Cardiol. 2000. 12:365–368.16. Kikuchi S, Hayashi Y, Fujioka S, Kukita H, Ochi N. A case of intracoronary stent implanted for acute myocardial infarction in an elderly patient with idiopathic thrombocytopenic purpura. Nippon Ronen Igakkai Zasshi. 2002. 39:88–93.17. Marques LG, Furukawa MK, Leitao TP, et al. Percutaneous transluminal coronary angioplasty in a patient with idiopathic thrombocytopenic purpura. Arq Bras Cardiol. 2005. 84:337–339.18. Stouffer GA, Hirmerova J, Moll S, et al. Percutaneous coronary intervention in a patient with immune thrombocytopenia purpura. Catheter Cardiovasc Interv. 2004. 61:364–367.
