Advanced peri-implantitis cases with radical surgical treatment
- Affiliations
-
- 1The Dental Implant and Gingival-Plastic Surgery Centre, Bournemouth, UK. shanemccrea@aol.com
- KMID: 1845882
- DOI: http://doi.org/10.5051/jpis.2014.44.1.39
Abstract
- PURPOSE
Peri-implantitis, a clinical term describing the inflammatory process that affects the soft and hard tissues around an osseointegrated implant, may lead to peri-implant pocket formation and loss of supporting bone. However, this imprecise definition has resulted in a wide variation of the reported prevalence; > or =10% of implants and 20% of patients over a 5- to 10-year period after implantation has been reported. The individual reporting of bone loss, bleeding on probing, pocket probing depth and inconsistent recording of results has led to this variation in the prevalence. Thus, a specific definition of peri-implantitis is needed. This paper describes the vast variation existing in the definition of peri-implantitis and suggests a logical way to record the degree and prevalence of the condition. The evaluation of bone loss must be made within the concept of natural physiological bony remodelling according to the initial peri-implant hard and soft tissue damage and actual definitive load of the implant. Therefore, the reason for bone loss must be determined as either a result of the individual osseous remodelling process or a response to infection.
METHODS
The most current Papers and Consensus of Opinion describing peri-implantitis are presented to illustrate the dilemma that periodontologists and implant surgeons are faced with when diagnosing the degree of the disease process and the necessary treatment regime that will be required.
RESULTS
The treatment of peri-implantitis should be determined by its severity. A case of advanced peri-implantitis is at risk of extreme implant exposure that results in a loss of soft tissue morphology and keratinized gingival tissue.
CONCLUSIONS
Loss of bone at the implant surface may lead to loss of bone at any adjacent natural teeth or implants. Thus, if early detection of peri-implantitis has not occurred and the disease process progresses to advanced peri-implantitis, the compromised hard and soft tissues will require extensive, skill-sensitive regenerative procedures, including implantotomy, established periodontal regenerative techniques and alternative osteotomy sites.
MeSH Terms
Figure
-

Figure 1 (A, B) Initial clinical presentation showing the extent of the buccal marginal gingival recession and the exposure of both root and implant surfaces. (C) Diagnostic panoramic radiograph. (D) Initial preoperative/diagnostic periapical radiograph showing the extent of bone loss at the implant and the adjacent canine tooth. The crown on the implant does not fit. (E) Linear tomogram showing the lack of hard tissue on the buccal aspect of the implant. (F) Diagonal mesial relieving incision. No relieving incision was made distal to the wound site. This flap design was chosen in anticipation of the large wound and increase in volume that would result from the graft materials and the need for increased sulcus vascularity for wound repair. A mucoperiosteal flap has been elevated to expose the extent of the defect. (G) The canine tooth was luxated first to allow for a complete assessment of the extent of bone loss associated with the implant. (H) The implant after luxation. Debridement of the defect was carried out, yet all marginal tissue was left intact to assist in wound coverage. The extent of the bone loss/defect was apparent at the lingual surface. (I) Bio-Gide membrane was placed at the lingual side between the lingual bony wall, but under the periosteum, to contain the subsequent Bio-Oss granules. (J) Bio-Oss granules (size, 0.25-1.00 mm) were placed into the voids to reform the bony morphology. (K) The Bio-Gide membrane was then folded over buccally to cover the Bio-Oss granules. The marginal granulations were placed over the membrane again. (L) The wound closure was facilitated with 5.0 Prolene sutures. (M). Periapical radiograph taken at 4 months post-operatively displaying the re-attainment of crestal bony margins and the filled in former void.
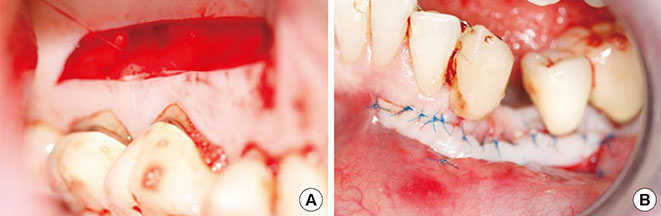
Figure 2 (A) At 4-month postimplantotomy, a split gingival graft was harvested from the left palatal vault. (B) Into the prepared buccal recipient site, the free split gingival graft was sutured into place using 6.0 Prolene sutures.
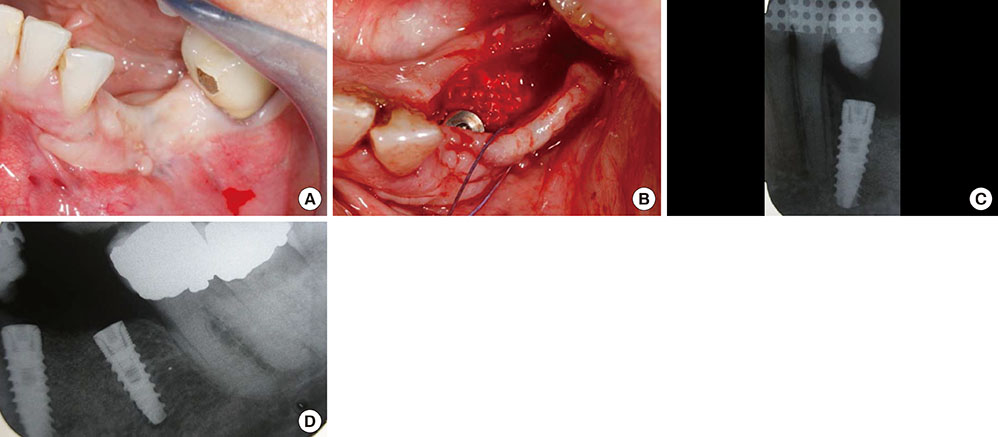
Figure 3 (A) The clinical situation before implant surgery and six months postimplantotomy. (B) A simple crestal incision was made, and reflection of the mucosa allows the exposure of the hard tissue formation for evaluation. Osteotomies were prepared in a centralized position on the crestal bone, and the implants were inserted with an initial seating torque value of 50 Ncm; final seating was carried out with a hand wrench at >50 Ncm. Additional Bio-Oss and the covering membrane were used to enhance the hard tissue volume at the site. Wound closure was carried out using 4.0 Vicryl sutures. (C, D) Immediate post-operative periapicals of the implants in place.

Figure 4 (A) Cervical margins of the implants just before the abutment fitting. (B) Cement-on fixed bridge in place. (C) Comparison of the surgically corrected left gingival margins with the natural tooth level on the right side. (D) Periapical radiograph taken 1-month postcementation.

Figure 5 (A) Clinical presentation at 36 months after fitting the bridge. (B) Periapical radiograph 36 months after procedure completion.

Figure 6 (A) Preoperative periapical radiograph. (B) Clinical situation immediately before implantotomy. (C) Mucoperiosteal flap reflection exposing the implant threads and fibrousfibrose tissue. (D) Fibrous tissue was removed to display the extent of the clinical bone loss. (E) The implant was removed and the site completely debrided prior to the placement of xenograft granules which were then covered with its dedicated membrane. (F) The wound was closed using 6.0 Prolene sutures.
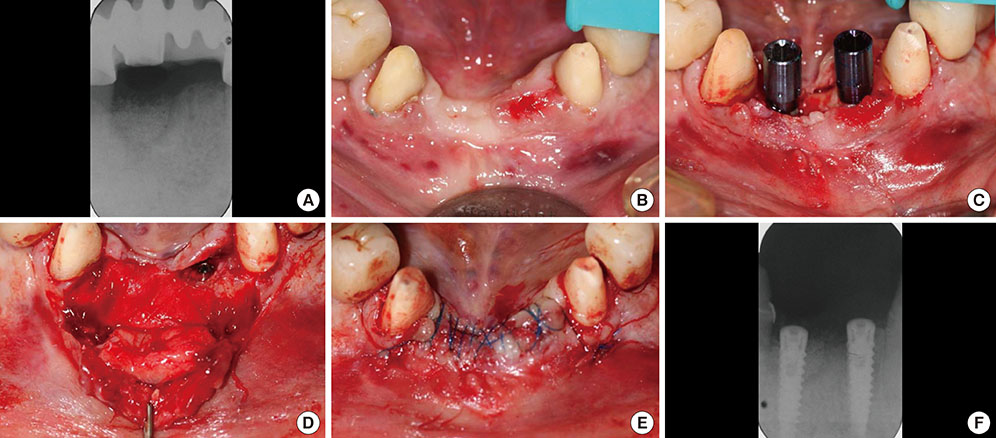
Figure 7 (A) Periapical radiograph taken 5 months postoperation. (B) Before the implant placement surgery and 5 months post implantotomy. (C) Osteotomies were prepared and the implants were placed centrally on the crestal bone in positions 41 and 31 (FDI-Notation), both with an initial seating torque of 50 Ncm; the final seating was carried out with a hand wrench at >50 Ncm. (D) Position 41 has been further 'grafted' with Bio-Oss granules and covered with its membrane to enhance the hard tissue volume at the site. Connective tissue was harvested from the palate and sutured to the underside of the mucoperiosteal flap using 6.0 Vicryl Rapide to prevent its exfoliation. (E) Wound closure via the coronal advancement of the labial flap using 5.0 Prolene sutures. (F) Periapical radiograph taken immediately postoperatively.
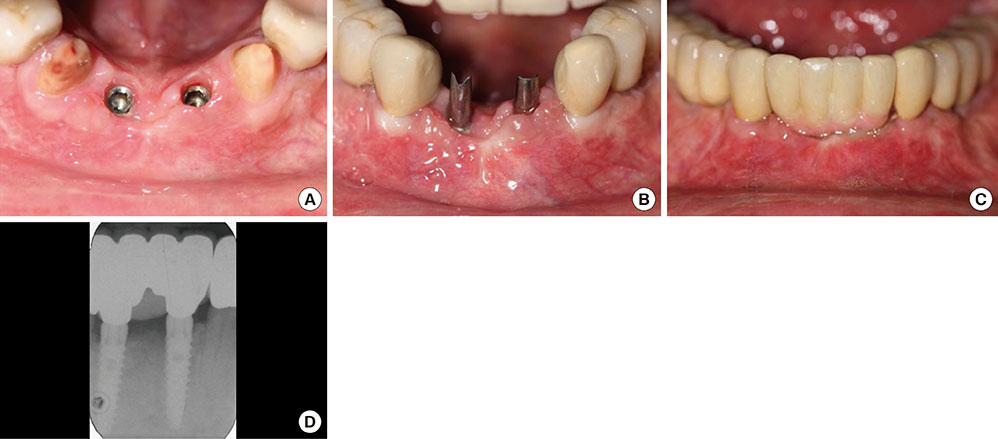
Figure 8 (A, B) Clinical presentation of the soft tissues six months postimplantation. (C) The fixed bridge was cemented onto the abutments. (D) Periapical radiograph taken 1-month postcementation.
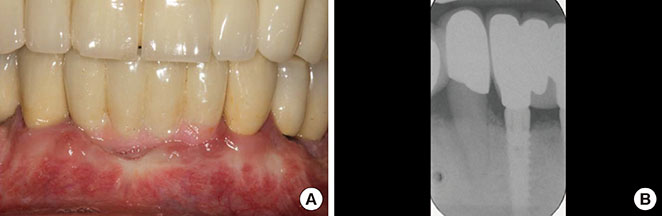
Figure 9 (A) Clinical presentation at 24-months after cementation of the bridge. (B) Periapical radiograph at 24-month postcementation.
Reference
-
1. Albrektsson T, Isidor F. Consensus report session IV. In : Lang NP, Kasrring T, editors. Proceedings of the First European Workshop on Periodontology. London: Quintessence;1994. p. 165–169.2. Klinge B, Meyle J. EAO consensus report: peri-implant tissue destruction. In : The Third EAO Consensus Conference 2012; 2012 Feb 15-18; Pfäffikon, Switzerland.3. Mombelli A, Muller N, Cionca N. The epidemiology of peri-implantitis. Clin Oral Implants Res. 2012; 23:Suppl 6. 67–76.
Article4. Roos-Jansaker AM, Lindahl C, Renvert H, Renvert S. Nine- to fourteen-year follow-up of implant treatment. Part II: presence of peri-implant lesions. J Clin Periodontol. 2006; 33:290–295.
Article5. Fransson C, Lekholm U, Jemt T, Berglundh T. Prevalence of subjects with progressive bone loss at implants. Clin Oral Implants Res. 2005; 16:440–446.
Article6. Ferreira SD, Silva GL, Cortelli JR, Costa JE, Costa FO. Prevalence and risk variables for peri-implant disease in Brazilian subjects. J Clin Periodontol. 2006; 33:929–935.
Article7. Koldsland OC, Scheie AA, Aass AM. Prevalence of peri-implantitis related to severity of the disease with different degrees of bone loss. J Periodontol. 2010; 81:231–238.
Article8. Jung RE, Pjetursson BE, Glauser R, Zembic A, Zwahlen M, Lang NP. A systematic review of the 5-year survival and complication rates of implant-supported single crowns. Clin Oral Implants Res. 2008; 19:119–130.
Article9. Berglundh T, Persson L, Klinge B. A systematic review of the incidence of biological and technical complications in implant dentistry reported in prospective longitudinal studies of at least 5 years. J Clin Periodontol. 2002; 29:Suppl 3. 197–212.
Article10. Froum SJ, Rosen PS. A proposed classification for peri-implantitis. Int J Periodontics Restorative Dent. 2012; 32:533–540.11. Karoussis IK, Kotsovilis S, Fourmousis I. A comprehensive and critical review of dental implant prognosis in periodontally compromised partially edentulous patients. Clin Oral Implants Res. 2007; 18:669–679.
Article12. Serino G, Wennstrom JL, Lindhe J, Eneroth L. The prevalence and distribution of gingival recession in subjects with a high standard of oral hygiene. J Clin Periodontol. 1994; 21:57–63.
Article13. Lindquist LW, Carlsson GE, Jemt T. Association between marginal bone loss around osseointegrated mandibular implants and smoking habits: a 10-year follow-up study. J Dent Res. 1997; 76:1667–1674.
Article14. Wennström J, Lindhe J. Role of attached gingiva for maintenance of periodontal health. Healing following excisional and grafting procedures in dogs. J Clin Periodontol. 1983; 10:206–221.
Article15. Wennstrom J, Lindhe J. Plaque-induced gingival inflammation in the absence of attached gingiva in dogs. J Clin Periodontol. 1983; 10:266–276.
Article16. Miyasato M, Crigger M, Egelberg J. Gingival condition in areas of minimal and appreciable width of keratinized gingiva. J Clin Periodontol. 1977; 4:200–209.
Article17. Lang NP, Loe H. The relationship between the width of keratinized gingiva and gingival health. J Periodontol. 1972; 43:623–627.
Article18. Dorfman HS, Kennedy JE, Bird WC. Longitudinal evaluation of free autogenous gingival grafts: a four year report. J Periodontol. 1982; 53:349–352.
Article19. Agudio G, Nieri M, Rotundo R, Cortellini P, Pini Prato G. Free gingival grafts to increase keratinized tissue: a retrospective long-term evaluation (10 to 25 years) of outcomes. J Periodontol. 2008; 79:587–594.
Article20. Agudio G, Nieri M, Rotundo R, Franceschi D, Cortellini P, Pini Prato GP. Periodontal conditions of sites treated with gingival-augmentation surgery compared to untreated contralateral homologous sites: a 10- to 27-year long-term study. J Periodontol. 2009; 80:1399–1405.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Risk factors of peri-implantitis: a narrative review
- Full mouth rehabilitation in a patient with peri-implantitis: A case report
- Combined surgical therapy for the treatment of combined supraand intrabony defects in peri-implantitis
- Unusual bone regeneration following resective surgery and decontamination of peri-implantitis: a 6-year follow-up
- Adjunctive use of Gel-type Desiccating Agent for Regenerative Surgical Treatment of Peri-implantitis in Patients with Inaccessible Implant Surface: A Case Report
