A Case of Chloroquine-Induced Cardiomyopathy That Presented as Sick Sinus Syndrome
- Affiliations
-
- 1Division of Cardiology, Department of Internal Medicine, College of Medicine, The Catholic University of Korea, Seoul, Korea. myleecardio@catholic.ac.kr
- 2Department of Radiology, College of Medicine, The Catholic University of Korea, Seoul, Korea.
- KMID: 1826182
- DOI: http://doi.org/10.4070/kcj.2010.40.11.604
Abstract
- A 52-year-old woman with rheumatoid arthritis who had been treated with prednisone and hydroxychloroquine for >12 years presented with chest discomfort and a seizure. She was diagnosed with restrictive cardiomyopathy combined with sick sinus syndrome. A myocardial muscle biopsy was performed to identify the underlying cardiomyopathy, which showed marked muscle fiber hypertrophy, fiber dropout, slightly increased interstitial fibrous connective tissue, and extensive cytoplasmic vacuolization of the myocytes under light microscopy. Electron microscopy of the myocytes demonstrated dense, myeloid, and curvilinear bodies. The diagnosis of hydroxychloroquine-induced cardiomyopathy was made based on the clinical, hemodynamic, and pathologic findings. This is the first case report describing chloroquine-induced cardiomyopathy involving the heart conduction system.
MeSH Terms
-
Arthritis, Rheumatoid
Biopsy
Cardiomyopathies
Cardiomyopathy, Restrictive
Connective Tissue
Cytoplasm
Female
Heart Conduction System
Hemodynamics
Humans
Hydroxychloroquine
Hypertrophy
Light
Microscopy
Microscopy, Electron
Middle Aged
Muscle Cells
Muscles
Patient Dropouts
Prednisone
Seizures
Sick Sinus Syndrome
Thorax
Hydroxychloroquine
Prednisone
Figure
-
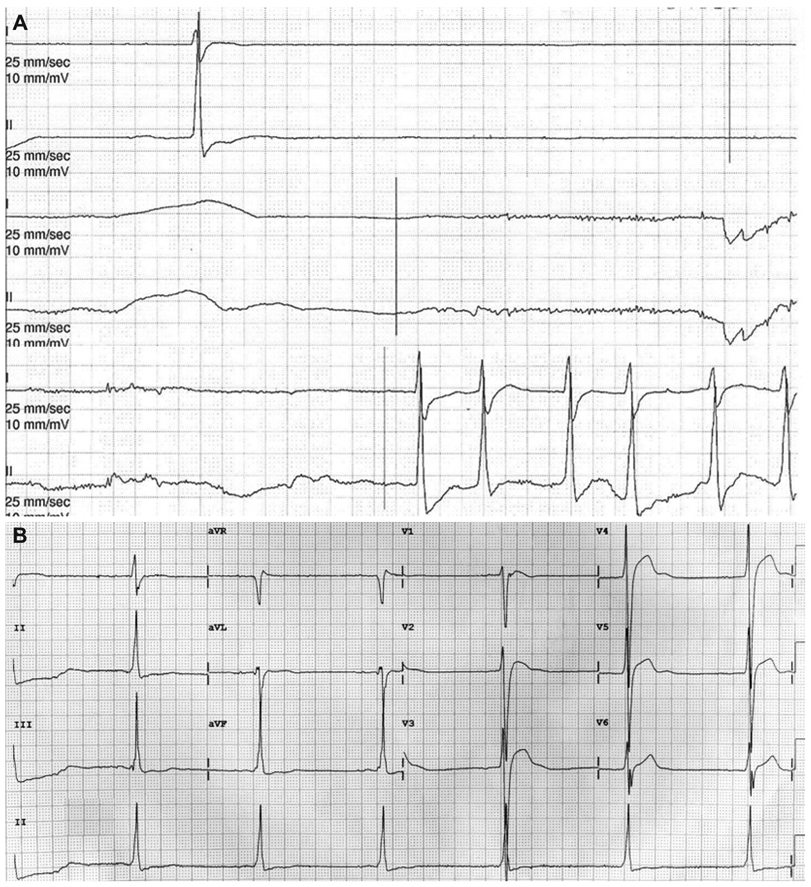
Fig. 1 Initial electrocardiogram findings. A: the rhythm strip shows sinus pause. B: the 12-lead electrocardiogram shows a junctional rhythm with sick sinus syndrome.
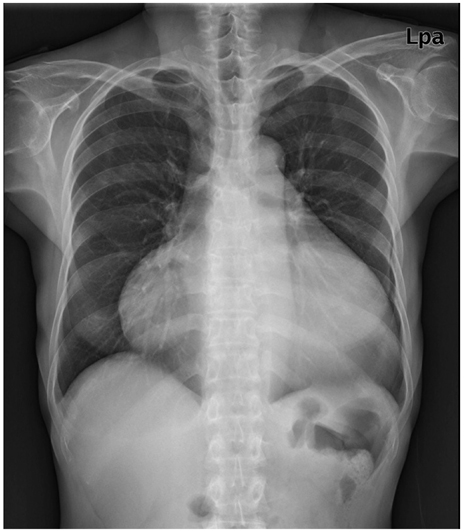
Fig. 2 Chest radiography demonstrated marked cardiomegaly without pulmonary congestion.

Fig. 3 Two-dimensional echocardiography reveals severe concentric LV hypertrophy, mild LV systolic dysfunction, a small pericardial effusion, and increased RV free wall thickness with mild RV systolic dysfunction. A: parasternal long axis view. B: parasternal short axis view at the mid-ventricular level. C: magnified apical 4-chamber view. D: mitral inflow view (E velocity, 90.28 cm/s; A velocity, 36.77 cm/s; deceleration time, 216.64 ms; E/E': 33.4). LV: left ventricular, RV: right ventricular.
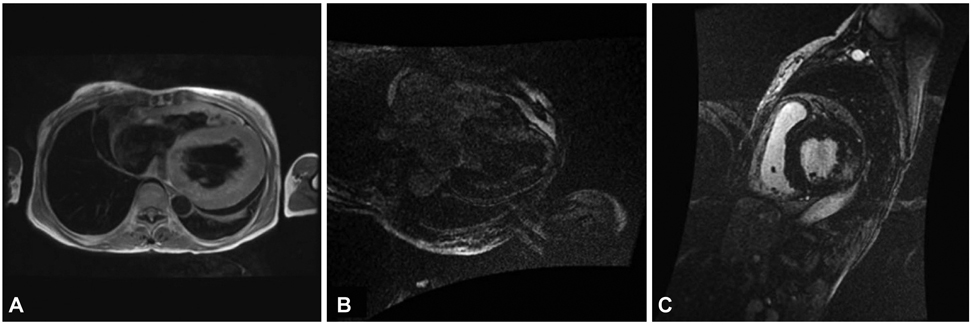
Fig. 4 Cardiac MRI findings. A: the black-blood coronal axis view on cardiac MRI demonstrates marked concentric left ventricle hypertrophy, suggesting hypertrophic cardiomyopathy. Right ventricle wall thickening is also noted and there is a small pericardial effusion. On delayed enhancement, signal hyperenhancement after gadolinium administration is observed within the septal wall on the coronal axis view (B) and lateral wall on the short axis view (C).
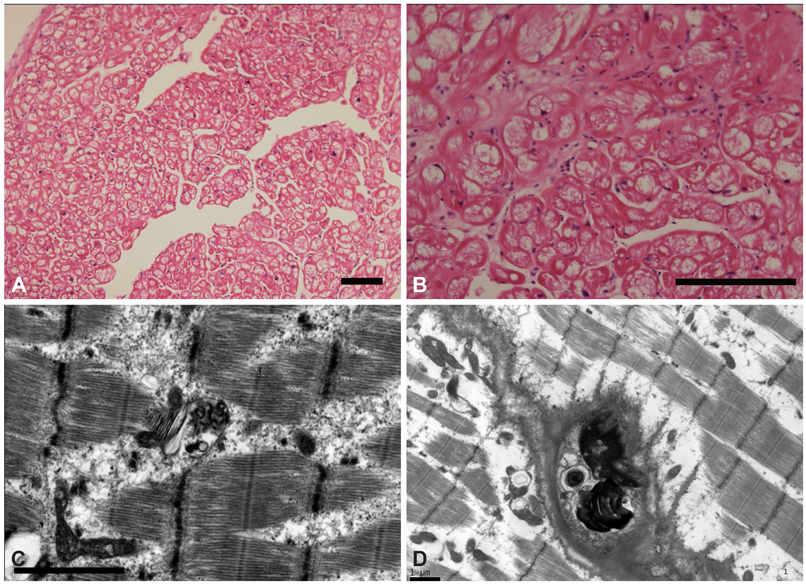
Fig. 5 Myocardial biopsy findings. A and B: light microscopy of the myocardial biopsy specimen showing diffusely enlarged myocytes with extensive cytoplasmic vacuolization (hematoxylineosin staining; A: original magnification ×100, B: ×200 scale bar, 200 µm). C: curvilinear bodies. This appearance is typical and characteristic of chloroquine and hydroxychloroquine toxicity. D: the transmission electron microscopy of the skeletal muscle biopsy specimen displays central replacement and displacement of the sarcomeres by marked accumulation of secondary lysosomes, including myeloid bodies (scale bar 1 µm).
Reference
-
1. Cervera A, Espinosa G, Font J, Ingelmo M. Cardiac toxicity secondary to long term treatment with chloroquine. Ann Rheum Dis. 2001. 60:301.2. Iglesias Cubero G, Rodrigue Reguero JJ, Rojo Ortega JM. Restrictive cardiomyopathy caused by chloroquine. Br Heart J. 1993. 69:451–452.3. Ratliff NB, Estes ML, Myles JL, Shirey EK, McMahon JT. Diagnosis of chloroquine cardiomyopathy by endomyocardial biopsy. N Engl J Med. 1987. 316:191–193.4. Weiner A, Sandberg MA, Gaudio AR, Kini MM, Berson EL. Hydroxychloroquine retinopathy. Am J Ophthalmol. 1991. 112:528–534.5. Hughes JT, Esiri M, Oxbury JM, Whitty CW. Chloroquine myopathy. Q J Med. 1971. 40:85–93.6. Estes ML, Ewing-Wilson D, Chou SM, et al. Chloroquine neuromyotoxicit: clinical and pathologic perspective. Am J Med. 1987. 82:447–455.7. Roos JM, Aubry MC, Edwards WD. Chloroquine cardiotoxicity: clinicopathologic features in three patients and comparison with three patients with Fabry disease. Cardiovasc Pathol. 2002. 11:277–283.8. Keating RJ, Bhatia S, Amin S, Williams A, Sinak LJ, Edwards WD. Hydroxychloroquine-induced cardiotoxicity in a 39-year-old woman with systemic lupus erythematosus and systolic dysfunction. J Am Soc Echocardiogr. 2005. 18:981.9. Rewcastle NB, Humphrey JG. Vacuolar myopathy: clinical, histochemical, and microscopic study. Arch Neurol. 1965. 12:570–582.10. Whisnant JP, Espinosa RE, Kierland RR, Lambert EH. Chloroquine neuromyopathy. Proc Staff Meet Mayo Clin. 1963. 38:501–513.11. Eadie MJ, Ferrier TM. Chloroquine myopathy. J Neurol Neurosurg Psychiatry. 1966. 29:331–337.12. Mastaglia FL, Papadimitriou JM, Dawkins RL, Beveridge B. Vacuolar myopathy associated with chloroquine, lupus erythematosus and thymoma: report of a case with unusual mitochondrial changes and lipid accumulation in muscle. J Neurol Sci. 1977. 34:315–328.13. Neville HE, Maunder-Sewry CA, McDougall J, Sewell JR, Dubowitz V. Chloroquine-induced cytosomes with curvilinear profiles in muscle. Muscle Nerve. 1979. 2:376–381.14. Gerard JM, Stoupel N, Collier A, Flament-Durand J. Morphologic study of a neuromyopathy caused by prolonged chloroquine treatment. Eur Neurol. 1973. 9:363–379.15. Fedorko ME, Hirsch JG, Cohn ZA. Autophagic vacuoles produced in vitro: II. studies on the mechanism of formation of autophagic vacuoles produced by chloroquine. J Cell Biol. 1968. 38:392–402.16. Macdonald RD, Engel AG. Experimental chloroquine myopathy. J Neuropathol Exp Neurol. 1970. 29:479–499.17. Motan J, Topinka I, Dura J, Kvapilova H. Chloroquine cardiodystrophy. Vnitr Lek. 1978. 24:1122–1128.18. Baguet JP, Tremel F, Fabre M. Chloroquine cardiomyopathy with conduction disorders. Heart. 1999. 81:221–223.19. Chung KY, Nam KB, Ko KK, et al. A case of idiopathic restrictive cardiomyopathy. Korean Circ J. 1990. 20:260–264.20. Bae EJ, Cheon EJ, Yun YS. Clinical profile and outcome of idiopathic restrictive cardiomyopathy in children. Korean Circ J. 2001. 31:427–433.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Familial Sick Sinus Syndrome
- Electrical Injury As A Possible Cause of Sick Sinus Syndrome
- A Case Report of Neuroleptanesthesia in a Parturient with Sick Sinus Syndrome
- Thyrotoxicosis Induced Sick Sinus Syndrome
- General Anesthesia with Laryngeal Mask Airway for Operation of a Patient with Sick - Sinus Syndrome
