Value of Additional Cervicothoracic Sagittal T2-Weighted Images in Elderly Patients with Symptoms Suggestive of Lumbar Spinal Stenosis
- Affiliations
-
- 1Department of Radiology, Seoul National University Bundang Hospital, Seongnam, Korea. joongmoahn@gmail.com
- KMID: 1823918
- DOI: http://doi.org/10.3348/jksr.2015.73.1.18
Abstract
- PURPOSE
The purpose of this study was to analyze the incidence and predictive factors of tandem cervical spinal stenosis (CSS) in patients with lumbar spinal stenosis (LSS) based on MR.
MATERIALS AND METHODS
From January to May of 2011, 140 consecutive patients (36 men, 94 women; mean age, 68.9 years; age range, 60-87 years) were included for the analysis. All patients were at least 60 years old, had undergone lumbar spine MRI including additional cervicothoracic sagittal T2-weighted images, and were clinically suspected of LSS. Two spine radiologists evaluated the risk factors for CSS, considering the possible risk factors such as age, sex, alignment disorder of the lumbar spine, number of levels of LSS, and severity of LSS, based on MR.
RESULTS
Of the 140 patients, 42 (30%) patients had tandem spinal stenosis. CSS was more common among patients with LSS (42 of 61, 69%) than among patients without LSS (27 of 79, 34%) (p = 0.000). Grade 2 or 3 CSS was more commonly observed among patients with grade 2 or 3 LSS (15 of 53, 28%), than among patients with grade 0 or 1 LSS (8 of 87, 9%) (p = 0.003). Only the severity of LSS showed a significant association with the severity of CSS (p = 0.045).
CONCLUSION
Tandem CSS is common in LSS, and the severity of LSS is a risk factor of CSS.
MeSH Terms
Figure
-
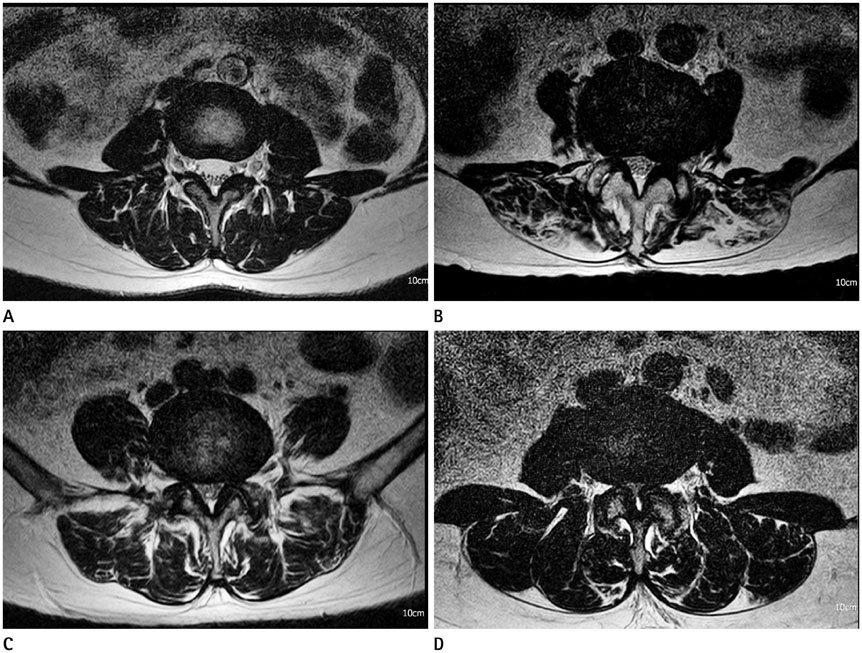
Fig. 1 Grading system of LSS using axial T2-weighted MR images. A. Grade 0, in which the anterior CSF space was not obliterated. B. Grade 1, in which the anterior CSF space was mildly obliterated but all cauda equina could be clearly separated from each other. C. Grade 2, in which the anterior CSF space was moderately obliterated and some of the cauda equina were aggregated, making it impossible to visually separate them. D. Grade 3, in which the anterior CSF space was obliterated severely as to show marked compression of the dural sac and none of the cauda equina could be visually separated from each other, appearing instead as one bundle. CSF = cerebrospinal fluid, LSS = lumbar spinal stenosis

Fig. 2 Grading system of CSS using sagittal T2-weighted images. Grade 0, in which D is greater than 50%. Grade 1, in which D is less than or equal to 50% and greater than 5%. Grade 2, in which D is less than or equal to 5% and greater than -5%. Grade 3, in which D is less than or equal to -5%. D = (C - B) / (A - B) × 100 (%) A: AP dimension of the non-stenotic central canal, B: AP dimension of the spinal cord, C: AP dimension of the stenotic central canal, D: Fraction of CSF reserve. AP = anteroposterior, CSF = cerebrospinal fluid, CSS = cervical spinal stenosis, LSS = lumbar spinal stenosis
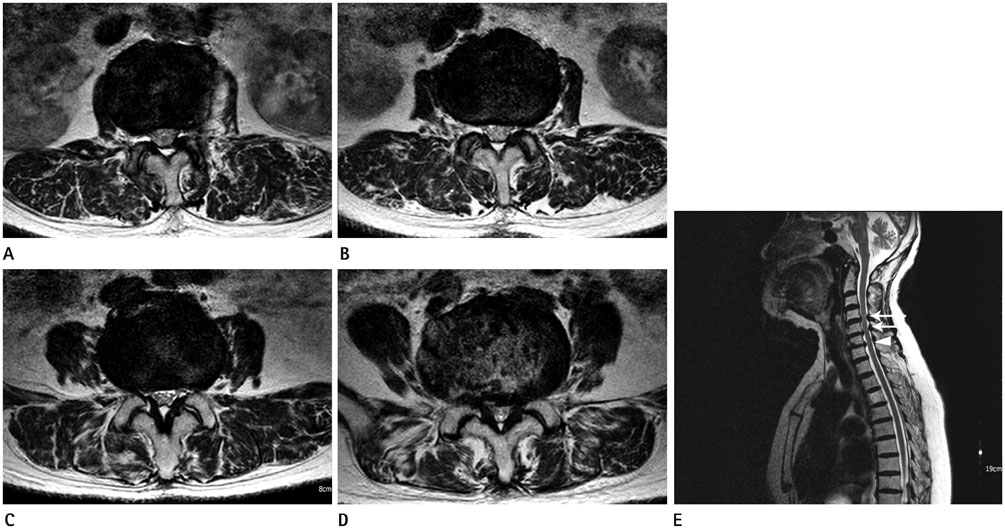
Fig. 3 An 83-year-old woman with claudication. A-D. Axial T2-weighted MR images show grade 1 central canal stenosis at L1-2 and L2-3 and grade 2 central canal stenosis at L3-4 and L4-5. E. The sagittal T2-weighted MR image demonstrates grade 2 central canal stenosis at C4-5 and C5-6 (arrows) and grade 1 central canal stenosis at C6-7 (arrowhead). Ossifications of ligamentum flavum are present at T8-9 and T9-10.
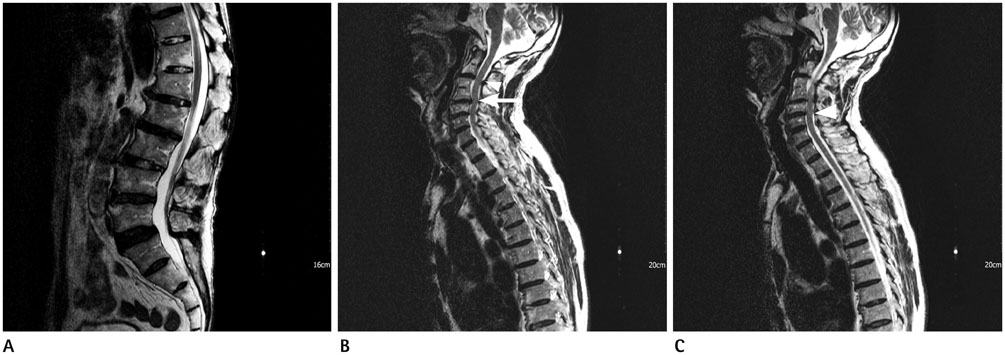
Fig. 4 A 73-year-old man with lower back pain. A. The sagittal T2-weighted MR image shows L5-S1 degenerative spondylolisthesis. There is no spinal stenosis at the lumbar spine. B, C. The sagittal T2-weighted MR image shows grade 2 central canal stenosis at C4-5 (arrow) and grade 1 central canal stenosis at C2-3 and C5-6 (arrowheads). A block vertebra is present at C3-4.
Reference
-
1. Teng P, Papatheodorou C. Combined cervical and lumbar spondylosis. Arch Neurol. 1964; 10:298–307.2. Dagi TF, Tarkington MA, Leech JJ. Tandem lumbar and cervical spinal stenosis. Natural history, prognostic indices, and results after surgical decompression. J Neurosurg. 1987; 66:842–884.3. LaBan MM, Green ML. Concurrent (tandem) cervical and lumbar spinal stenosis: a 10-yr review of 54 hospitalized patients. Am J Phys Med Rehabil. 2004; 83:187–190.4. Epstein NE, Epstein JA, Carras R, Murthy VS, Hyman RA. Coexisting cervical and lumbar spinal stenosis: diagnosis and management. Neurosurgery. 1984; 15:489–496.5. Aydogan M, Ozturk C, Mirzanli C, Karatoprak O, Tezer M, Hamzaoglu A. Treatment approach in tandem (concurrent) cervical and lumbar spinal stenosis. Acta Orthop Belg. 2007; 73:234–237.6. Harrison DE, Cailliet R, Harrison DD, Troyanovich SJ, Harrison SO. A review of biomechanics of the central nervous system--part II: spinal cord strains from postural loads. J Manipulative Physiol Ther. 1999; 22:322–332.7. Lee GY, Lee JW, Choi HS, Oh KJ, Kang HS. A new grading system of lumbar central canal stenosis on MRI: an easy and reliable method. Skeletal Radiol. 2011; 40:1033–1039.8. Hsieh CH, Huang TJ, Hsu RW. Tandem spinal stenosis: clinical diagnosis and surgical treatment. Changgeng Yi Xue Za Zhi. 1998; 21:429–435.9. Naderi S, Mertol T. Simultaneous cervical and lumbar surgery for combined symptomatic cervical and lumbar spinal stenoses. J Spinal Disord Tech. 2002; 15:229–231. discussion 231-23210. Kikuike K, Miyamoto K, Hosoe H, Shimizu K. One-staged combined cervical and lumbar decompression for patients with tandem spinal stenosis on cervical and lumbar spine: analyses of clinical outcomes with minimum 3 years follow-up. J Spinal Disord Tech. 2009; 22:593–601.11. Eskander MS, Aubin ME, Drew JM, Eskander JP, Balsis SM, Eck J, et al. Is there a difference between simultaneous or staged decompressions for combined cervical and lumbar stenosis? J Spinal Disord Tech. 2011; 24:409–413.12. Thomé C, Börm W, Meyer F. Degenerative lumbar spinal stenosis: current strategies in diagnosis and treatment. Dtsch Arztebl Int. 2008; 105:373–379.13. Lee SH, Kim KT, Suk KS, Lee JH, Shin JH, So DH, et al. Asymptomatic cervical cord compression in lumbar spinal stenosis patients: a whole spine magnetic resonance imaging study. Spine (Phila Pa 1976). 2010; 35:2057–2206.14. Lee MJ, Garcia R, Cassinelli EH, Furey C, Riew KD. Tandem stenosis: a cadaveric study in osseous morphology. Spine J. 2008; 8:1003–1006.15. Sirvanci M, Bhatia M, Ganiyusufoglu KA, Duran C, Tezer M, Ozturk C, et al. Degenerative lumbar spinal stenosis: correlation with Oswestry Disability Index and MR imaging. Eur Spine J. 2008; 17:679–685.16. Muhle C, Metzner J, Weinert D, Falliner A, Brinkmann G, Mehdorn MH, et al. Classification system based on kinematic MR imaging in cervical spondylitic myelopathy. AJNR Am J Neuroradiol. 1998; 19:1763–1771.17. Slipman CW, Shin CH, Patel RK, Isaac Z, Huston CW, Lipetz JS, et al. Etiologies of failed back surgery syndrome. Pain Med. 2002; 3:200–214. discussion 214-217
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Value of Additional Cervicothoracic Spine Sagittal T2-weighted Images Included in Routine Lumbar Spine MR Imaging
- Clinical Utility of Limited T2-Weighted-Only Lumbar Spine MRI in Pain Intervention Clinics
- Should We Recommend Ultrasonography for an Incidental Thyroid Nodule on Additional Cervicothoracic Sagittal T2-Weighted Image of Lumbar Spine MRI?
- Coexisting Spine Lesions on Whole Spine T2 Sagittal MRI in Evaluating Spinal Degenerative Disease
- Asymptomatic Cervical or Thoracic Lesions in Elderly Patients who Have Undergone Decompressive Lumbar Surgery for Stenosis
