Ann Surg Treat Res.
2015 Feb;88(2):69-76. 10.4174/astr.2015.88.2.69.
A comparative analysis of endoscopic thyroidectomy versus conventional thyroidectomy in clinically lymph node negative thyroid cancer
- Affiliations
-
- 1Department of Surgery, Konkuk University School of Medicine, Seoul, Korea. ks2002p@hanmail.net
- KMID: 1804123
- DOI: http://doi.org/10.4174/astr.2015.88.2.69
Abstract
- PURPOSE
Differentiated thyroid cancer has a good prognosis and high incidence in young women. Since endoscopic techniques were first recorded in 1996, surgical indications of endoscopic thyroidectomy have broadened. Therefore, the aim of this study is to investigate the usefulness of endoscopic thyroidectomy in clinically lymph node negative (cN0) thyroid cancer patients, based on oncologic completeness and safety, considering cosmetic outcomes.
METHODS
From July 2009 to June 2011, a total of 166 cases had undergone endoscopic thyroidectomy using the BABA (bilateral axillo-breast approach) method or conventional open thyroidectomy by one surgeon. Finally, excluding 72 patients, 94 patients with cN0 thyroid cancer were divided into two groups according to operative methods and analyzed to compare differences between the two methods retrospectively (endoscopic group, n = 49; conventional open group, n = 45).
RESULTS
We practiced comparative analysis for clinicopathologic characteristics, surgical outcomes including postoperative complications, and recurred cases during follow-up periods of each group. The results showed there was a tendency for patients, young, women rather than men, and having small size of thyroid cancer, to prefer endoscopic surgery to open surgery. Meanwhile, in postoperative complications, there were no statistically significant differences. During short follow-up periods, no recurrence or mortality case was observed.
CONCLUSION
Endoscopic thyroidectomy is a feasible and safe method for the treatment of clinically lymph node negative (cN0) thyroid cancer.
MeSH Terms
Figure
-
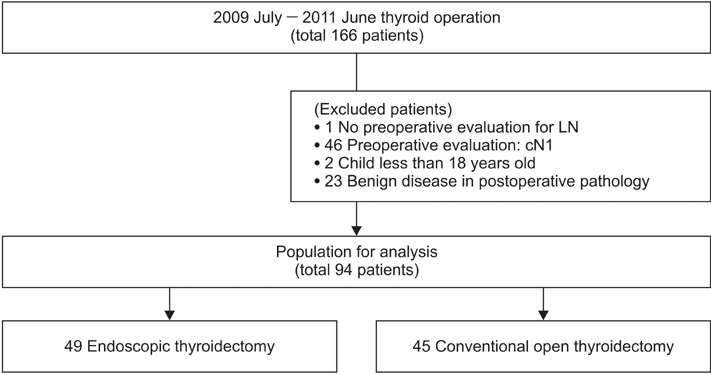
Fig. 1 Flow chart of accrued patients. LN, lymph node.
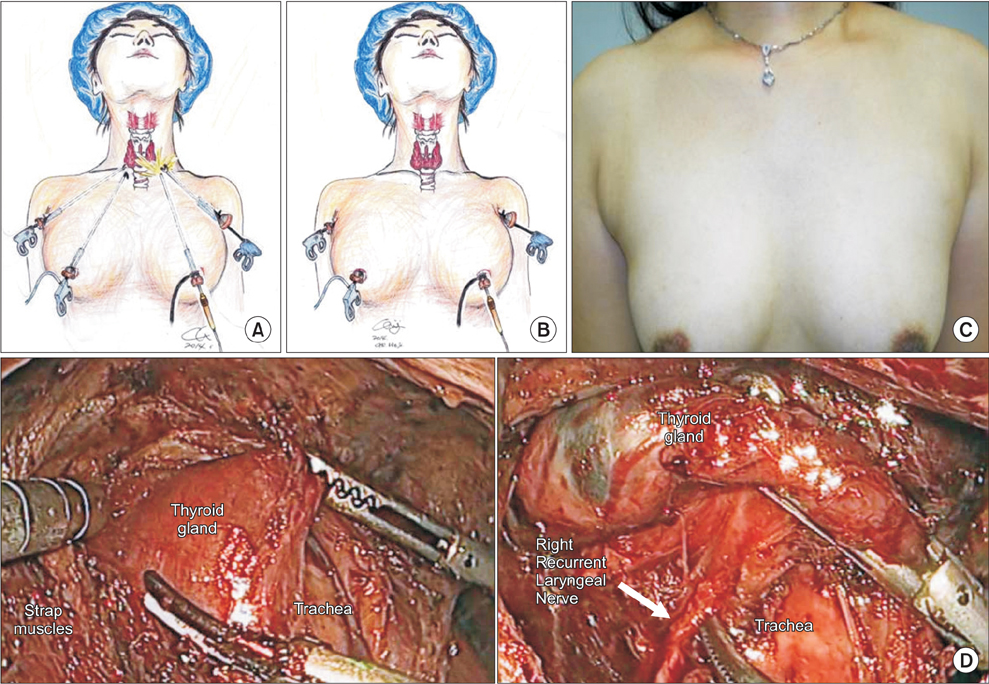
Fig. 2 Endoscopic thyroidectomy using the BABA (bilateral axillo-breast approach) method; (A) intraoperative scope insertion, (B) actual surgical approach, (C) outcome at 2nd week postoperatively, and (D) intraoperative picture (anatomy).
Reference
-
1. Yang L, Shen W, Sakamoto N. Population-based study evaluating and predicting the probability of death resulting from thyroid cancer and other causes among patients with thyroid cancer. J Clin Oncol. 2013; 31:468–474.2. Liu M, Ruan M, Chen L. Update on the molecular diagnosis and targeted therapy of thyroid cancer. Med Oncol. 2014; 31:973.3. Barney BM, Hitchcock YJ, Sharma P, Shrieve DC, Tward JD. Overall and cause-specific survival for patients undergoing lobectomy, near-total, or total thyroidectomy for differentiated thyroid cancer. Head Neck. 2011; 33:645–649.4. Cramer JD, Fu P, Harth KC, Margevicius S, Wilhelm SM. Analysis of the rising incidence of thyroid cancer using the Surveillance, Epidemiology and End Results national cancer data registry. Surgery. 2010; 148:1147–1152.5. Moon EK, Park HJ, Oh CM, Jung KW, Shin HY, Park BK, et al. Cancer incidence and survival among adolescents and young adults in Korea. PLoS One. 2014; 9:e96088.6. Horn-Ross PL, Lichtensztajn DY, Clarke CA, Dosiou C, Oakley-Girvan I, Reynolds P, et al. Continued rapid increase in thyroid cancer incidence in california: trends by patient, tumor, and neighborhood characteristics. Cancer Epidemiol Biomarkers Prev. 2014; 23:1067–1079.7. Vergamini LB, Frazier AL, Abrantes FL, Ribeiro KB, Rodriguez-Galindo C. Increase in the incidence of differentiated thyroid carcinoma in children, adolescents, and young adults: a population-based study. J Pediatr. 2014; 164:1481–1485.8. Shaw A, Semenciw R, Mery L. Cancer in Canada fact sheet series #1 - thyroid cancer in Canada. Chronic Dis Inj Can. 2014; 34:64–68.9. Shin HR, Jung KW, Won YJ, Park JG. 2002 annual report of the Korea Central Cancer Registry: based on registered data from 139 hospitals. Cancer Res Treat. 2004; 36:103–114.10. Lee KE, Choi JY, Youn YK. Bilateral axillo-breast approach robotic thyroidectomy. Surg Laparosc Endosc Percutan Tech. 2011; 21:230–236.11. Aidan P, Pickburn H, Monpeyssen H, Boccara G. Indications for the gasless transaxillary robotic approach to thyroid surgery: experience of forty-seven procedures at the american hospital of paris. Eur Thyroid J. 2013; 2:102–109.12. Lee J, Chung WY. Robotic surgery for thyroid disease. Eur Thyroid J. 2013; 2:93–101.13. Choi JY, Lee KE, Chung KW, Kim SW, Choe JH, Koo do H, et al. Endoscopic thyroidectomy via bilateral axillo-breast approach (BABA): review of 512 cases in a single institute. Surg Endosc. 2012; 26:948–955.14. Chung YS, Choe JH, Kang KH, Kim SW, Chung KW, Park KS, et al. Endoscopic thyroidectomy for thyroid malignancies: comparison with conventional open thyroidectomy. World J Surg. 2007; 31:2302–2306.15. Im HJ, Koo DH, Paeng JC, Lee KE, Chung YS, Lim I, et al. Evaluation of surgical completeness in endoscopic thyroidectomy compared with open thyroidectomy with regard to remnant ablation. Clin Nucl Med. 2012; 37:148–151.16. Bae DS, Koo DH, Choi JY, Kim E, Lee KE, Youn YK. Current status of robotic thyroid surgery in South Korea: a web-based survey. World J Surg. 2014; 38:2632–2639.17. Jemal A, Bray F, Center MM, Ferlay J, Ward E, Forman D. Global cancer statistics. CA Cancer J Clin. 2011; 61:69–90.18. Daliri M, Abbaszadegan MR, Bahar MM, Arabi A, Yadollahi M, Ghafari A, et al. The role of BRAF V600E mutation as a potential marker for prognostic stratification of papillary thyroid carcinoma: a long-term follow-up study. Endocr Res. 2014; 39:189–193.19. Hughes DT, Haymart MR, Miller BS, Gauger PG, Doherty GM. The most commonly occurring papillary thyroid cancer in the United States is now a microcarcinoma in a patient older than 45 years. Thyroid. 2011; 21:231–236.20. Muenscher A, Dalchow C, Kutta H, Knecht R. The endoscopic approach to the neck: a review of the literature, and overview of the various techniques. Surg Endosc. 2011; 25:1358–1363.21. Gal I, Solymosi T, Szabo Z, Balint A, Bolgar G. Minimally invasive video-assisted thyroidectomy and conventional thyroidectomy: a prospective randomized study. Surg Endosc. 2008; 22:2445–2449.22. Piniek A, Schuhmann R, Coerper S. Minimally invasive video-assisted thyroidectomy: establishment in a thyroid center. Chirurg. 2014; 85:246–252.23. Nixon IJ, Ganly I, Patel SG, Morris LG, Palmer FL, Thomas D, et al. Observation of clinically negative central compartment lymph nodes in papillary thyroid carcinoma. Surgery. 2013; 154:1166–1172.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Endoscopic Thyroidectomy in Thyroid Cancer
- A Clinical Application of Gasless Endoscopic Thyroidectomy: Clinical Analysis of 300 Cases at a Single Institution
- Thyroid Lobectomy as an Initial Treatment Option on 1-4 cm Papillary Cancer
- The Significance of Internal Jugular Node Sampling in Well-Differentiated Thyroid Cancer
- Transaxillary Endoscopic Thyroidectomy versus Conventional Open Thyroidectomy for Papillary Thyroid Cancer: 5-year Surgical Outcomes
