Korean J Gastroenterol.
2012 May;59(5):347-353. 10.4166/kjg.2012.59.5.347.
Usefulness of 18F-fluoro-2-deoxyglucose Positron Emission Tomography in Evaluation of Gastric Cancer Stage
- Affiliations
-
- 1Department of Internal Medicine, The Catholic University of Korea, College of Medicine, Seoul, Korea. parkjerry@catholic.ac.kr
- 2Department of Surgery, The Catholic University of Korea, College of Medicine, Seoul, Korea.
- KMID: 1792833
- DOI: http://doi.org/10.4166/kjg.2012.59.5.347
Abstract
- BACKGROUND/AIMS
The usefulness of 18F-fluoro-2-deoxyglucose (FDG)-PET in detecting primary cancer, lymph node metastasis, and distant metastasis were studied in the gastric cancer patients.
METHODS
The subjects were 392 gastric cancer patients who received FDG-PET and an abdominal CT test prior to surgery. The results of FDG-PET and CT were compared with the surgical and pathologic results.
RESULTS
The primary site detection rate of FDG-PET was 74.4%, 50.3% in early gastric cancer and 92.0% in advanced gastric cancer. Detection rate was higher when tumors were larger than 3.5 cm, had deeper depth of invasion, and at a later stage (p<0.05, respectively). In multivariate analysis, tumor size, spread of tumor cells beyond the muscle layer (> or =T2), and lymph node metastasis were statistically significant factors in primary site detection rate. The sensitivity, specificity, and positive predictive value of FDG-PET to lymph node metastasis were 59.6%, 88.8%, and 81.1% respectively, sensitivity being lower compared to CT while specificity and positive predictive value were higher. Sensitivity, specificity, and positive predictive value to distant metastasis were, respectively, 66.7%, 99.2%, and 88.0%, similar to CT. In 21 of the 392 patients (5.4%), synchronous double primary cancers were detected.
CONCLUSIONS
In gastric cancer, usefullness of FDG-PET is limited to the advanced stage. Diagnostic value of this test was not superior to CT. However, FDG-PET may be useful in detecting synchronous double primary cancers.
Keyword
MeSH Terms
-
Aged
Female
Fluorodeoxyglucose F18/chemistry/*diagnostic use
Humans
Lymphatic Metastasis
Male
Middle Aged
Neoplasm Staging
Positron-Emission Tomography
Predictive Value of Tests
ROC Curve
Radiopharmaceuticals/chemistry/*diagnostic use
Retrospective Studies
Stomach Neoplasms/*diagnosis/radionuclide imaging
Tomography, X-Ray Computed
Figure
-
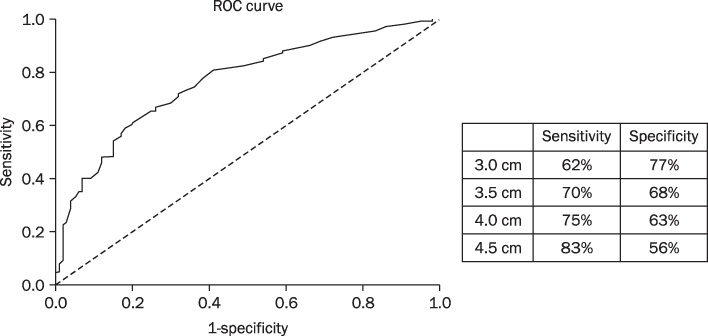
Fig. 1 Detection rate of gastric cancer with 18F-fluoro-2-deoxyglucose (FDG)-PET according to tumor size. ROC, receiver operating characteristic.
Reference
-
1. Han EJ, Choi WH, Chung YA, et al. Comparison between FDG uptake and clinicopathologic and immunohistochemical parameters in pre-operative PET/CT scan of primary gastric carcinoma. Nucl Med Mol Imaging. 2009. 43:26–34.2. Bar-Shalom R, Valdivia AY, Blaufox MD. PET imaging in oncology. Semin Nucl Med. 2000. 30:150–185.3. Yeung HW, Macapinlac H, Karpeh M, Finn RD, Larson SM. Accuracy of FDG-PET in gastric cancer. Preliminary experience. Clin Positron Imaging. 1998. 1:213–221.4. Koga H, Sasaki M, Kuwabara Y, et al. An analysis of the physiological FDG uptake pattern in the stomach. Ann Nucl Med. 2003. 17:733–738.5. Terauchi T, Murano T, Daisaki H, et al. Evaluation of whole-body cancer screening using 18F-2-deoxy-2-fluoro-D-glucose positron emission tomography: a preliminary report. Ann Nucl Med. 2008. 22:379–385.6. Kim SK, Kang KW, Lee JS, et al. Assessment of lymph node metastases using 18F-FDG PET in patients with advanced gastric cancer. Eur J Nucl Med Mol Imaging. 2006. 33:148–155.7. Japanese Gastric Cancer Association. Japanese classification of gastric carcinoma-2nd English edition. Gastric Cancer. 1998. 1:10–24.8. Hamilton SR, Aaltonen LA. Tumors of the stomach. WHO classification of tumors. Pathology and genetics. Tumors of the digestive system. 2000. Lyon: IARC Press;38–52.9. Sobin LH, Wittekind C. International Union Against Cancer (UICC): TNM classification of malignant tumours. 2002. 6th ed. New York: Wiley-Liss;65–68.10. Podoloff DA, Ball DW, Ben-Josef E, et al. NCCN task force: clinical utility of PET in a variety of tumor types. J Natl Compr Canc Netw. 2009. 7:Suppl 2. S1–S26.11. Yamada A, Oguchi K, Fukushima M, Imai Y, Kadoya M. Evaluation of 2-deoxy-2-[18F]fluoro-D-glucose positron emission tomography in gastric carcinoma: relation to histological subtypes, depth of tumor invasion, and glucose transporter-1 expression. Ann Nucl Med. 2006. 20:597–604.12. Stahl A, Ott K, Weber WA, et al. FDG PET imaging of locally advanced gastric carcinomas: correlation with endoscopic and histopathological findings. Eur J Nucl Med Mol Imaging. 2003. 30:288–295.13. Chen J, Cheong JH, Yun MJ, et al. Improvement in preoperative staging of gastric adenocarcinoma with positron emission tomography. Cancer. 2005. 103:2383–2390.14. Mukai K, Ishida Y, Okajima K, Isozaki H, Morimoto T, Nishiyama S. Usefulness of preoperative FDG-PET for detection of gastric cancer. Gastric Cancer. 2006. 9:192–196.15. Mochiki E, Kuwano H, Katoh H, Asao T, Oriuchi N, Endo K. Evaluation of 18F-2-deoxy-2-fluoro-D-glucose positron emission tomography for gastric cancer. World J Surg. 2004. 28:247–253.16. Peeters CF, de Waal RM, Wobbes T, Ruers TJ. Metastatic dormancy imposed by the primary tumor: does it exist in humans? Ann Surg Oncol. 2008. 15:3308–3315.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- 18F-2-Deoxy-2-Fluoro-D-Glucose Positron Emission Tomography: Computed Tomography for Preoperative Staging in Gastric Cancer Patients
- Role of 18F 2-fluoro-2-deoxyglucose Positron Emission Tomography in Upper Gastrointestinal Malignancies
- Effectiveness of 18F-fluoro-deoxyglucose Positron Emission Tomography/Computed Tomography and Magnetic Resonance Imaging to Detect Iliopsoas Tendonitis after Total Hip Arthroplasty: A Case Report
- Basic principles and applications of 18F-FDG-PET/CT in oral and maxillofacial imaging: A pictorial essay
- Positron Emission Tomography: Application in Pediatric Epilepsy
