New Parameters for Left Ventricular Function in Atrial Fibrillation: Based on the Relationship between RR Interval and Performance
- Affiliations
-
- 1Division of Cardiology, Department of Internal Medicine, College of Medicine, Chung-Ang University, Seoul, Korea. cjkim@cau.ac.kr
- KMID: 1781718
- DOI: http://doi.org/10.3346/jkms.2005.20.1.20
Abstract
- This study was designed to obtain new parameters representing left ventricular (LV) function independent of irregular RR intervals in atrial fibrillation (AF). AF patients were divided into Normal (n=9) and LV Dysfunction (n=9) groups. The relations between LV outflow peak ejection velocity (Vpe) and preceding (RR-1) or prepreceding RR intervals (RR-2) were obtained using logarithmic equations, from which the squared correlation coefficient (r2), slope, Vpe at RR-1 or RR-2=1 sec (Vpe-1), and the ratio of slope to Vpe-1 (Slope/Vpe-1) were calculated. Among the parameters between RR-1 and Vpe, Slope/Vpe-1 was higher in LV Dysfunction group than in Normal group (p=0.05). When only coordinates with RR-1 from 0.6 to 1 sec were included, Slope/Vpe-1 (p=0.001) was higher in LV Dysfunction group than in Normal group. Among the parameters between RR-2 and Vpe, Slope/Vpe-1, slope, and r2 were different between the two groups. In multivariate analysis, Slope/Vpe-1 between RR-2 and Vpe was only independent parameter. However, Slope/Vpe-1 between RR-1 and Vpe in the coordinates with RR-1 from 0.6 to 1 sec had the highest discriminating power. New parameters derived from the relations between RR intervals and LV performance might be useful to evaluate LV function quantitatively in AF.
MeSH Terms
-
Age Factors
Aged
Atrial Fibrillation/*metabolism
Atrial Function, Left
Echocardiography
Echocardiography, Doppler, Pulsed
Electrocardiography
Female
Heart/physiology
Heart Ventricles
Hemodynamic Processes
Humans
Male
Middle Aged
Models, Theoretical
Multivariate Analysis
Myocardial Contraction
Myocardium/pathology
Time Factors
*Ventricular Function, Left
Figure
-

Fig. 1 Differences of new parameters representing LV function between Normal and LV Dysfunction groups in atrial fibrillation. (A) Slope/Vpe-1 in the relation between RR-2 and Vpe, (B) Slope/Vpe-1 in the relation between RR-1 and Vpe and (C) Slope/Vpe-1 in the relation between RR-1 and Vpe in the coordinates with RR-1 from 0.6 to 1 sec.
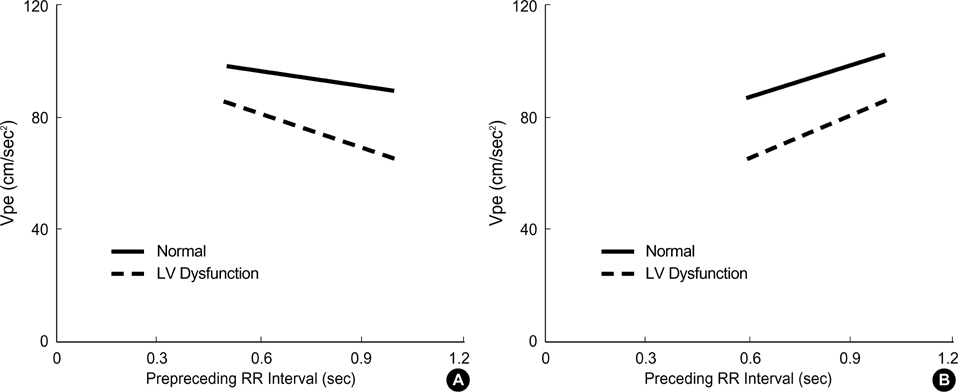
Fig. 2 The relations between (A) pre-preceding RR interval (RR-2) or (B) preceding RR interval (RR-1) and LV performance (Vpe) in Normal and LV Dysfunction groups.

Fig. 3 The relations between fractional shortening and new parameters representing LV function in atrial fibrillation. (A) Slope/Vpe-1 in the relation between RR-2 and Vpe, and (B) Slope/Vpe-1 in the relation between RR-1 and Vpe in coordinates with RR-1 from 0.6 to 1 sec.
Reference
-
1. Daoud EG, Weiss R, Bahu M, Knight BP, Bogun F, Goyal R, Harvey M, Strickberger SA, Man KC, Morady F. Effect of an irregular ventricular rhythm on cardiac output. Am J Cardiol. 1996. 78:1433–1436.
Article2. Clark DM, Plumb VJ, Epstein AE, Kay GN. Hemodynamic effects of an irregular sequence of ventricular cycle lengths during atrial fibrillation. J Am Coll Cardiol. 1997. 30:1039–1045.
Article3. Effat M, Schick EC, Martin DT, Gaasch WH. Effect of rhythm regularization on left ventricular contractility in patients with atrial fibrillation. Am J Cardiol. 2000. 85:114–116.
Article4. Gosselink AT, Blanksma PK, Crijns HJ, Van Gelder IC, de Kam PJ, Hillege HL, Niemeijer MG, Lie KI, Meijler FL. Left ventricular beat-to-beat performance in atrial fibrillation: contribution of Frank-Starling mechanism after short rather than long RR intervals. J Am Coll Cardiol. 1995. 26:1516–1521.
Article5. Muntinga HJ, Gosselink AT, Blanksma PK, De Kam PJ, Van Der Wall EE, Crijns HJ. Left ventricular beat to beat performance in atrial fibrillation: dependence on contractility, preload, and afterload. Heart. 1999. 82:575–580.
Article6. Hardman SM, Noble MI, Biggs T, Seed WA. Evidence for an influence of mechanical restitution on beat-to-beat variations in haemodynamics during chronic atrial fibrillation in patients. Cardiovasc Res. 1998. 38:82–90.
Article7. Hardman SM, Noble MI, Seed WA. Postextrasystolic potentiation and its contribution to the beat-to-beat variation of the pulse during atrial fibrillation. Circulation. 1992. 86:1223–1232.
Article8. Rawles JM. A mathematical model of left ventricular function in atrial fibrillation. Int J Biomed Comput. 1988. 23:57–68.
Article9. Pfeiffer KP, Kenner T, Schaefer J. Application of statistical methods for the analysis or interval related cardiac performance variations during cardiac arrhythmia in man. Cardiovasc Res. 1984. 18:80–98.
Article10. Dubrey SW, Falk RH. Optimal number of beats for the Doppler measurement of cardiac output in atrial fibrillation. J Am Soc Echocardiogr. 1997. 10:67–71.
Article11. Takagaki M, McCarthy PM, Chung M, Connor J, Dessoffy R, Ochiai Y, Howard M, Doi K, Kopcak M, Mazgalev TN, Fukamachi K. Preload-adjusted maximal power: a novel index of left ventricular contractility in atrial fibrillation. Heart. 2002. 88:170–176.
Article12. Freeman GL, Colston JT. Evaluation of left ventricular mechanical restitution in closed-chest dogs based on single-beat elastance. Circ Res. 1990. 67:1437–1445.
Article13. Schneider F, Martin DT, Schick EC, Gaasch WH. Interval-dependent changes in left ventricular contractile state in lone atrial fibrillation and in atrial fibrillation associated with coronary artery disease. Am J Cardiol. 1997. 80:586–590.
Article14. Kerr AJ, Simmonds MB, Stewart RA. Influence of heart rate on stroke volume variability in atrial fibrillation in patients with normal and impaired left ventricular function. Am J Cardiol. 1998. 82:1496–1500.
Article15. Ko HS, Lee KJ, Kim SW, Kim TH, Kim CJ, Ryu WS. Prediction of left ventricular peak ejection velocity by preceding and prepreceding RR intervals in atrial fibrillation: A new method to adjust the influence between two intervals. J Korean Med Sci. 2002. 17:743–748.16. Sahn DJ, DeMaria A, Kisslo J, Weyman A. Recommendations regarding quantitation in M-mode echocardiography: results of a survey of echocardiographic measurements. Circulation. 1978. 58:1072–1083.
Article17. Brookes CI, White PA, Staples M, Oldershaw PJ, Redington AN, Collins PD, Noble MI. Myocardial contractility is not constant during spontaneous atrial fibrillation in patients. Circulation. 1998. 98:1762–1768.
Article18. Grogan M, Smith HC, Gersh BJ, Wood DL. Left ventricular dysfunction due to atrial fibrillation in patients initially believed to have idiopathic dilated cardiomyopathy. Am J Cardiol. 1992. 69:1570–1573.
Article19. Packer DL, Bardy GH, Worley SJ, Smith MS, Cobb FR, Coleman RE, Gallagher JJ, German LD. Tachycardia-induced cardiomyopathy: a reversible form of left ventricular dysfunction. Am J Cardiol. 1986. 57:563–570.
Article20. Nagahama Y, Schick EC, Gaasch WH. Interval-dependent potentiation of left ventricular contractility is preserved in patients with atrial fibrillation and depressed ejection fraction. Am J Cardiol. 2001. 87:342–346.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Prediction of Left Ventricular Peak Ejection Velocity by Preceding and Prepreceding RR Intervals in Atrial fibrillation:A New Method to Adjust the Influence between Two Intervals
- Relation Between RR Intervals and Early Diastolic Mitral Annular Velocities in Atrial Fibrillation
- The Relationship between Preceding RR Intervals and Peak Ejection Velocity of Left Ventricular Outflow in Atrial Fibrillation without Organic Heart Diseases
- Relationship Between RR Intervals and Early Diastolic Mitral Annulus Velocities in Atrial Fibrillation Patients Who do not Have Significant Valvular Diseases
- Atrial Fibrillation in a Patient with Left Ventricular Hypertrophy after Induction of General Anesthesia: A case report
