J Korean Med Sci.
2007 Jun;22(3):470-475. 10.3346/jkms.2007.22.3.470.
Basal Serum Cortisol Levels are not Predictive of Response to Corticotropin but Have Prognostic Significance in Patients with Septic Shock
- Affiliations
-
- 1Division of Pulmonary and Critical Care Medicine, Department of Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, 50 Irwon-dong, Gangnam-gu, Seoul, Korea. gysuh@smc.samsung.co.kr
- 2Department of Pulmonary and Critical Care Medicine, Division of Internal Medicine, College of Medicine, Korea University Anam Hospital, Seoul, Korea.
- KMID: 1778356
- DOI: http://doi.org/10.3346/jkms.2007.22.3.470
Abstract
- Because high levels of cortisol are frequently observed in patients with septic shock, low levels of serum cortisol are considered indicative of relative adrenal insufficiency (RAI). This study was performed to investigate whether pretest clinical characteristics, including basal serum cortisol levels, are predictive of serum cortisol response to corticotropin and whether basal cortisol levels have a prognostic significance in patients with septic shock. We performed a retrospective analysis of 68 patients with septic shock who underwent short corticotropin stimulation testing. RAI was defined as an increase in cortisol level <9 microgram/dL from baseline, and results showed that 48 patients (70.6%) had this insufficiency. According to the univariate analysis, the RAI group had significantly higher simplified acute physiology score II (SAPS II) and sequential organ failure assessment (SOFA) scores than the non-RAI group. The incidence of RAI was the same regardless of the basal serum cortisol level (p=0.447). The hospital mortality rate was 58.8% and was not significantly different between the RAI and non-RAI groups. However, a high basal serum cortisol level (> or =30 microgram/dL) was significantly associated with in-hospital mortality. In conclusion, our data suggest that basal serum cortisol levels are not predictive of serum cortisol response to corticotropin but have a significant prognostic value in patients with septic shock.
Keyword
MeSH Terms
Figure
-
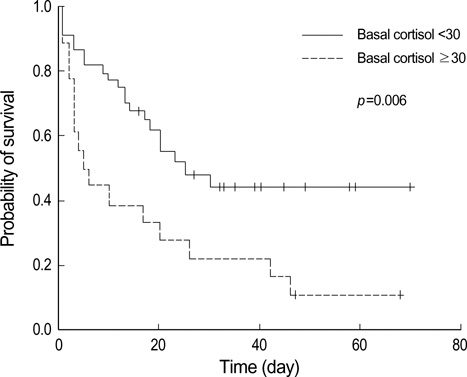
Fig. 1 Kaplan-Meier analysis of the survival probability in patients with septic shock.
Cited by 2 articles
-
A Prospective Study on the Incidence and Predictive Factors of Relative Adrenal Insufficiency in Korean Critically-Ill Patients
Yong Soo Kwon, Eunhae Kang, Gee Young Suh, Won-Jung Koh, Man Pyo Chung, Hojoong Kim, O Jung Kwon, Jae Hoon Chung
J Korean Med Sci. 2009;24(4):668-673. doi: 10.3346/jkms.2009.24.4.668.Prognostic Implication of Adrenocortical Response during the Course of Critical Illness
Jin Hwa Song, Jung Hee Kim, Sang-Min Lee, Jinwoo Lee
Acute Crit Care. 2019;34(1):38-45. doi: 10.4266/acc.2018.00339.
Reference
-
1. Schein RM, Sprung CL, Marcial E, Napolitano L, Chernow B. Plasma cortisol levels in patients with septic shock. Crit Care Med. 1990. 18:259–263.
Article2. Besse JC, Bass AD. Potentiation by hydrocortisone of responses to catecholamines in vascular smooth muscle. J Pharmacol Exp Ther. 1966. 154:224–238.3. Iversen LL, Salt PJ. Inhibition of catecholamine Uptake-2 by steroids in the isolated rat heart. Br J Pharmacol. 1970. 40:528–530.
Article4. Kalsner S. Mechanism of hydrocortisone potentiation of responses to epinephrine and norepinephrine in rabbit aorta. Circ Res. 1969. 24:383–395.
Article5. Annane D, Sebille V, Troche G, Raphael JC, Gajdos P, Bellissant E. A 3-level prognostic classification in septic shock based on cortisol levels and cortisol response to corticotropin. JAMA. 2000. 283:1038–1045.
Article6. Annane D, Sebille V, Charpentier C, Bollaert PE, Francois B, Korach JM, Capellier G, Cohen Y, Azoulay E, Troche G, Chaumet-Riffaut P, Bellissant E. Effect of treatment with low doses of hydrocortisone and fludrocortisone on mortality in patients with septic shock. JAMA. 2002. 288:862–871.
Article7. Sibbald WJ, Short A, Cohen MP, Wilson RF. Variations in adrenocortical responsiveness during severe bacterial infections. Unrecognized adrenocortical insufficiency in severe bacterial infections. Ann Surg. 1977. 186:29–33.8. Hamrahian AH, Oseni TS, Arafah BM. Measurements of serum free cortisol in critically ill patients. N Engl J Med. 2004. 350:1629–1638.
Article9. Molijn GJ, Spek JJ, van Uffelen JC, de Jong FH, Brinkmann AO, Bruining HA, Lamberts SW, Koper JW. Differential adaptation of glucocorticoid sensitivity of peripheral blood mononuclear leukocytes in patients with sepsis or septic shock. J Clin Endocrinol Metab. 1995. 80:1799–1803.
Article10. Cooper MS, Stewart PM. Corticosteroid insufficiency in acutely ill patients. N Engl J Med. 2003. 348:727–734.
Article11. Manglik S, Flores E, Lubarsky L, Fernandez F, Chhibber VL, Tayek JA. Glucocorticoid insufficiency in patients who present to the hospital with severe sepsis: a prospective clinical trial. Crit Care Med. 2003. 31:1668–1675.
Article12. Marik PE, Zaloga GP. Adrenal insufficiency during septic shock. Crit Care Med. 2003. 31:141–145.
Article13. Salluh JI, Verdeal JC, Mello GW, Araujo LV, Martins GA, de Sousa Santino M, Soares M. Cortisol levels in patients with severe community-acquired pneumonia. Intensive Care Med. 2006. 32:595–598.
Article14. Annane D, Bellissant E, Sebille V, Lesieur O, Mathieu B, Raphael JC, Gajdos P. Impaired pressor sensitivity to noradrenaline in septic shock patients with and without impaired adrenal function reserve. Br J Clin Pharmacol. 1998. 46:589–597.
Article15. Hoen S, Asehnoune K, Brailly-Tabard S, Mazoit JX, Benhamou D, Moine P, Edouard AR. Cortisol response to corticotropin stimulation in trauma patients: influence of hemorrhagic shock. Anesthesiology. 2002. 97:807–813.16. American College of Chest Physicians/Society of Critical Care Medicine Consensus Conference: definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis. Crit Care Med. 1992. 20:864–874.17. Oelkers W. Adrenal insufficiency. N Engl J Med. 1996. 335:1206–1212.
Article18. Grinspoon SK, Biller BM. Clinical review 62: Laboratory assessment of adrenal insufficiency. J Clin Endocrinol Metab. 1994. 79:923–931.
Article19. Oelkers W, Diederich S, Bahr V. Diagnosis and therapy surveillance in Addison's disease: rapid adrenocorticotropin (ACTH) test and measurement of plasma ACTH, renin activity, and aldosterone. J Clin Endocrinol Metab. 1992. 75:259–264.
Article20. Erturk E, Jaffe CA, Barkan AL. Evaluation of the integrity of the hypothalamic-pituitary-adrenal axis by insulin hypoglycemia test. J Clin Endocrinol Metab. 1998. 83:2350–2354.
Article21. Beishuizen A, Thijs LG. Relative adrenal failure in intensive care: an identifiable problem requiring treatment? Best Pract Res Clin Endocrinol Metab. 2001. 15:513–531.
Article22. Oelkers W. Dose-response aspects in the clinical assessment of the hypothalamo-pituitary-adrenal axis, and the low-dose adrenocorticotropin test. Eur J Endocrinol. 1996. 135:27–33.
Article23. Zaloga GP, Marik P. Hypothalamic-pituitary-adrenal insufficiency. Crit Care Clin. 2001. 17:25–41.
Article24. Burke CW. Adrenocortical insufficiency. Clin Endocrinol Metab. 1985. 14:947–976.
Article25. Burchard K. A review of the adrenal cortex and severe inflammation: quest of the "eucorticoid" state. J Trauma. 2001. 51:800–814.
Article26. Lamberts SW, Bruining HA, de Jong FH. Corticosteroid therapy in severe illness. N Engl J Med. 1997. 337:1285–1292.
Article27. Jurney TH, Cockrell JL Jr, Lindberg JS, Lamiell JM, Wade CE. Spectrum of serum cortisol response to ACTH in ICU patients. Correlation with degree of illness and mortality. Chest. 1987. 92:292–295.28. Wade CE, Lindberg JS, Cockrell JL, Lamiell JM, Hunt MM, Ducey J, Jurney TH. Upon-admission adrenal steroidogenesis is adapted to the degree of illness in intensive care unit patients. J Clin Endocrinol Metab. 1988. 67:223–227.
Article29. Rothwell PM, Lawler PG. Prediction of outcome in intensive care patients using endocrine parameters. Crit Care Med. 1995. 23:78–83.
Article30. Dellinger RP, Carlet JM, Masur H, Gerlach H, Calandra T, Cohen J, Gea-Banacloche J, Keh D, Marshall JC, Parker MM, Ramsay G, Zimmerman JL, Vincent JL, Levy MM. Surviving Sepsis Campaign guidelines for management of severe sepsis and septic shock. Crit Care Med. 2004. 32:858–873.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Significance of Corticosteroids and Their Relationship with Other Parameters in Patients with Sepsis
- Comparison of salivary and serum cortisol levels in mechanically ventilated patients and non-critically ill patients
- What Are the Predictive Factors of Severe Conditions in Acute Obstructive Pyelonephritis?
- Responese of Serum Prolactin, Growth Hormone and Cortisol to Generalized Epileptic Seizures and to Stress
- Stimulated Salivary Cortisol as a Noninvasive Diagnostic Tool for Adrenal Insufficiency
