Effect of Heart Rate and Coronary Calcification on the Diagnostic Accuracy of the Dual-Source CT Coronary Angiography in Patients with Suspected Coronary Artery Disease
- Affiliations
-
- 1Shandong Province Ji'nan 4th People's Hospital, Ji'nan 250031, China.
- 2Department of Cardiology, Shandong Provincial Hospital, Ji'nan 250021, China. cuilianqun@163.com
- 3School of Medicine, Shandong University, Ji'nan 250012, China.
- KMID: 1777262
- DOI: http://doi.org/10.3348/kjr.2009.10.4.347
Abstract
OBJECTIVE
To evaluate the diagnostic accuracy of a dual-source computed tomography (DSCT) coronary angiography, with a particular focus on the effect of heart rate and calcifications.
MATERIALS AND METHODS
One hundred and nine patients with suspected coronary disease were divided into 2 groups according to a mean heart rate (< 70 bpm and > or = 70 bpm) and into 3 groups according to the mean Agatston calcium scores (< or = 100, 101-400, and > 400). Next, the effect of heart rate and calcification on the accuracy of coronary artery stenosis detection was analyzed by using an invasive coronary angiography as a reference standard. Coronary segments of less than 1.5 mm in diameter in an American Heart Association (AHA) 15-segment model were independently assessed.
RESULTS
The mean heart rate during the scan was 71.8 bpm, whereas the mean Agatston score was 226.5. Of the 1,588 segments examined, 1,533 (97%) were assessable. A total of 17 patients had calcium scores above 400 Agatston U, whereas 50 had heart rates > or = 70 bpm. Overall the sensitivity, specificity, positive predictive values (PPV) and negative predictive values (NPV) for significant stenoses were: 95%, 91%, 65%, and 99% (by segment), respectively and 97%, 90%, 81%, and 91% (by artery), respectively (n = 475). Heart rate showed no significant impact on lesion detection; however, vessel calcification did show a significant impact on accuracy of assessment for coronary segments. The specificity, PPV and accuracy were 96%, 80%, and 96% (by segment), respectively for an Agatston score less than 100% and 99%, 96% and 98% (by artery). For an Agatston score of greater to or equal to 400 the specificity, PPV and accuracy were reduced to 79%, 55%, and 83% (by segment), respectively and to 79%, 69%, and 85% (by artery), respectively.
CONCLUSION
The DSCT provides a high rate of accuracy for the detection of significant coronary artery disease, even in patients with high heart rates and evidence of coronary calcification. However, patients with severe coronary calcification (> 400 U) remain a challenge to diagnose.
MeSH Terms
Figure
-
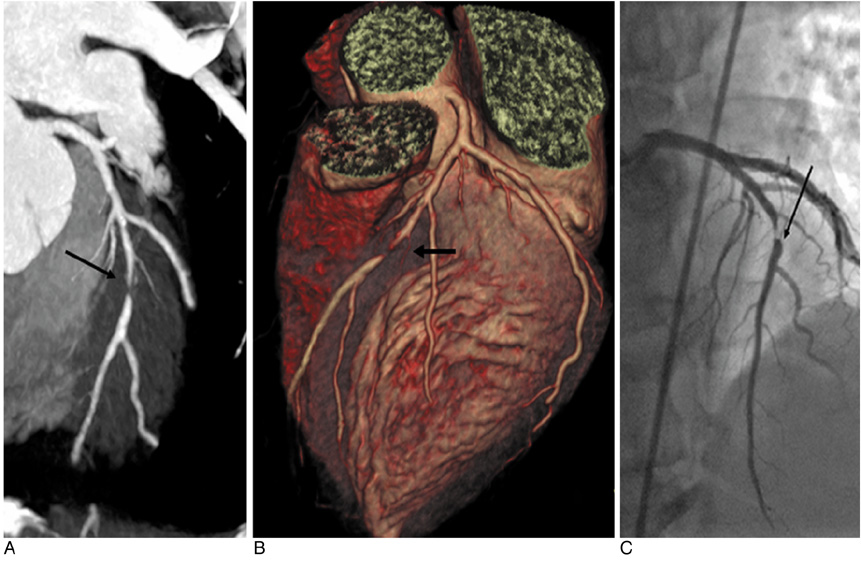
Fig. 1 Dual-source CT coronary angiography in 50-year-old man with suspected coronary artery disease (mean heart rate 88 bpm). Curved-planar maximum-intensity projections (A) and three-dimensional volume rendering technique reconstructions (B) of left anterior descending artery both demonstrate significant artery stenosis of mid segment (arrow). Patient has one-vessel disease. Invasive coronary angiography (C) confirms significant stenosis of mid segment of right coronary artery (arrow).

Fig. 2 Dual-source CT coronary angiography in 50-year-old man with suspected coronary artery disease (Agatston score 823). Curved-planar maximum-intensity projections (A) of left anterior descending artery demonstrate significant stenosis of proximal and mid segment (arrow). However, invasive coronary angiography (B) in right anterior oblique cranial view shows mild to moderate degree of lumen reduction (< 50%) in proximal and mid segment (arrow) of left anterior descending artery, resulting in false positive diagnosis in dual-source CT coronary angiography. Patient has three-vessel disease and shows diffused calcification in left circumflex artery and right coronary artery (figure not shown).
Reference
-
1. Ohnesorge B, Flohr T, Becker C, Kopp AF, Schoepf UJ, Baum U, et al. Cardiac imaging by means of electrocardiographically gated multisection spiral CT: initial experience. Radiology. 2000. 217:564–571.2. Kachelriess M, Ulzheimer S, Kalender WA. ECG-correlated image reconstruction from subsecond multi-slice spiral CT scans of the heart. Med Phys. 2000. 27:1881–1902.3. Taguchi K, Anno H. High temporal resolution for multislice helical computed tomography. Med Phys. 2000. 27:861–872.4. Becker CR, Knez A, Leber A, Hong C, Treede H, Wildhirt S, et al. Initial experiences with multislice detector spiral CT in diagnosis of arteriosclerosis of coronary vessels. Radiologe. 2000. 40:118–122.5. Achenbach S, Ulzheimer S, Baum U, Kachelriess M, Ropers D, Giesler T, et al. Noninvasive coronary angiography by retrospectively ECG-gated multislice spiral CT. Circulation. 2000. 102:2823–2828.6. Nieman K, Oudkerk M, Rensing BJ, van Ooijen P, Munne A, van Geuns RJ, et al. Coronary angiography with multislice computed tomography. Lancet. 2001. 357:599–603.7. Achenbach S, Giesler T, Ropers D, Ulzheimer S, Derlien H, Schulte C, et al. Detection of coronary artery stenoses by contrast-enhanced, retrospectively ECG-gated, multislice spiral CT. Circulation. 2001. 103:2535–2538.8. Knez A, Becker CR, Leber A, Ohnesorge B, Becker A, White C, et al. Usefulness of multislice spiral computed tomography angiography for determination of coronary artery stenoses. Am J Cardiol. 2001. 88:1191–1194.9. Raff GL, Gallagher MJ, O'Neill WW, Goldstein JA. Diagnostic accuracy of noninvasive angiography using 64-slice spiral computed tomography. J Am Coll Cardiol. 2005. 46:552–557.10. Hoffmann MH, Shi H, Schmitz BL, Schmid FT, Lieberknecht M, Schulze R, et al. Noninvasive coronary angiography with multislice computed tomography. JAMA. 2005. 293:2471–2478.11. Achenbach S, Ropers D, Kuettner A, Flohr T, Ohnesorge B, Bruder H, et al. Contrast-enhanced coronary artery visualization by dual-source computed tomography-initial experience. Eur J Radiol. 2006. 57:331–335.12. Johnson TR, Nikolaou K, Wintersperger BJ, Leber AW, von Ziegler F, Rist C, et al. Dual-source CT cardiac imaging: initial experience. Eur Radiol. 2006. 16:1409–1415.13. Scheffel H, Alkadhi H, Plass A, Vachenauer R, Desbiolles L, Gaemperli O, et al. Accuracy of dual-source CT coronary angiography: first experience in a high pre-test probability population without heart rate control. Eur Radiol. 2006. 16:2739–2747.14. Flohr TG, McCollough CH, Bruder H, Petersilka M, Gruber K, Süss C, et al. First performance evaluation of a dual-source CT (DSCT) system. Eur Radiol. 2006. 16:256–268.15. Zhang Z, Jin Z, Zhang S, Lin S, Li D, Kong L, et al. Coronary artery imaging with dual-source CT: initial experience. Chin J Radiol. 2007. 41:973–976.16. Austen WG, Edwards JE, Frye RL, Gensini GG, Gott VL, Griffith LS, et al. A reporting system on patients evaluated for coronary artery disease. Report of the Ad Hoc Committee for Grading of Coronary Artery Disease, Council on Cardiovascular Surgery, American Heart Association. Circulation. 1975. 51:5–40.17. Ehara M, Surmely JF, Kawai M, Katoh O, Matsubara T, Terashima M, et al. Diagnostic accuracy of 64-slice computed tomography for detecting angiographically significant coronary artery stenosis in an unselected consecutive patient population: comparison with conventional invasive angiography. Circ J. 2006. 70:564–571.18. Giesler T, Baum U, Ropers D, Ulzheimer S, Wenkel E, Mennicke M, et al. Noninvasive visualization of coronary arteries using contrast-enhanced multidetector CT: influence of heart rate on image quality and stenosis detection. AJR Am J Roentgenol. 2002. 179:911–916.19. Schroeder S, Kopp AF, Kuettner A, Burgstahler C, Herdeg C, Heuschmid M, et al. Influence of heart rate on vessel visibility in noninvasive coronary angiography using new multislice computed tomography: experience in 94 patients. Clin Imaging. 2002. 26:106–111.20. Hoffmann MH, Shi H, Manzke R, Schmid FT, De Vries L, Grass M, et al. Noninvasive coronary angiography with 16-detector row CT: effect of heart rate. Radiology. 2005. 234:86–97.21. Ong TK, Chin SP, Liew CK, Chan WL, Seyfarth MT, Liew HB, et al. Accuracy of 64-row multidetector computed tomography in detecting coronary artery disease in 134 symptomatic patients: influence of calcification. Am Heart J. 2006. 151:1323.22. Brodoefel H, Reimann A, Burgstahler C, Schumacher F, Herberts T, Tsiflikas I, et al. Noninvasive coronary angiography using 64-slice spiral computed tomography in an unselected patient collective: effect of heart rate, heart rate variability and coronary calcifications on image quality and diagnostic accuracy. Eur J Radiol. 2008. 66:134–141.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Coronary CT Angiography
- Current Progress of Studies of Coronary CT for Risk Prediction of Major Adverse Cardiovascular Event (MACE)
- Spontaneous Coronary Artery Dissection and Woven Coronary Artery: Three Cases and a Review of the Literature
- Noninvasive Detection of Coronary Atherosclerotic Plaques and Assessment of Stenosis Degree at Multidetector CT Coronary Angiography
- Utility of Quantification of Coronary Artery Calcification Using Spiral CT
