Noninvasive Detection of Coronary Atherosclerotic Plaques and Assessment of Stenosis Degree at Multidetector CT Coronary Angiography
- Affiliations
-
- 1Department of Radiology, Sungkyunkwan University School of Medicine, Korea. yhchoe@smc.samsung.co.kr
- KMID: 2137783
- DOI: http://doi.org/10.5124/jkma.2007.50.2.109
Abstract
- 64-slice MDCT has shown a sensitivity of 86 ~ 99% and a specificity of 79 ~ 96% in detecting lesions >50% stenosis. Spatial resolution of current MDCT technology enables reliable detection of nonobstructing noncalcific plaques as well as significantly stenotic lesions. CT densitometry on the plaques may give an insight on vulnerability of the lesions defined as less than 30~50 HU. MDCT coronary angiography has a tendency of overestimation of stenosis degree especially in distal segments of left anterior descending and circumflex arteries and their branches and in heavily calcified lesions as compared with quantitative catheter coronary angiography. Semi-automatic vessel segmentation techniques for coronary CT angiography may help assess the stenosis degree quantitatively. Recently developed dual-source 128-slice CT has shown diagnostic quality images in patients with high heart rates. Along with forth-coming 256-slice CT, new CT technologies are expected to enable highly reliable detection of coronary artery plaques and accurate estimation of stenosis degree.
MeSH Terms
Figure
-

Figure 1 64-year-old woman with chest pain. Volume-rendered (A) and maximum intensity projection (B) images of 64-slice CT show mild stenosis (arrows) in proximal left anterior descending branch. Short-axial reformatted image (C) of the lesion shows an eccentric noncalcific plaque (arrow). Mean ROI of the plaque region was 46 HU suggestive of lipid-rich content in the plaque.

Figure 2 64-year-old male with chest pain. Volume-rendered (A) and maximum intensity projection (B) images show stenosis (arrow) in the proximal left anterior descending branch, first diagonal branch and ramus intermedius. Short-axial reformatted image (C) shows eccentric plaques (arrows) in these vessels. Also note hypo-attenuated areas (arrowheads) suggestive of lipid content. Plaque volume was measured using a semiautomated method (D). It showed that plaque consisted of mostly fibrous component (50~130 HU) and the volume of the plaque was 13.13mm3.
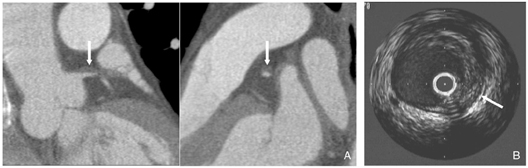
Figure 3 48-year-old male with acute myocardial infarction. CT reformatted images (A) show a noncalcific plaque (arrow) in left main coronary artery. Intravascular ultrasonography (B) confirmed presence of fibrous plaque (arrow) without foci of hypoechoic lipid component.
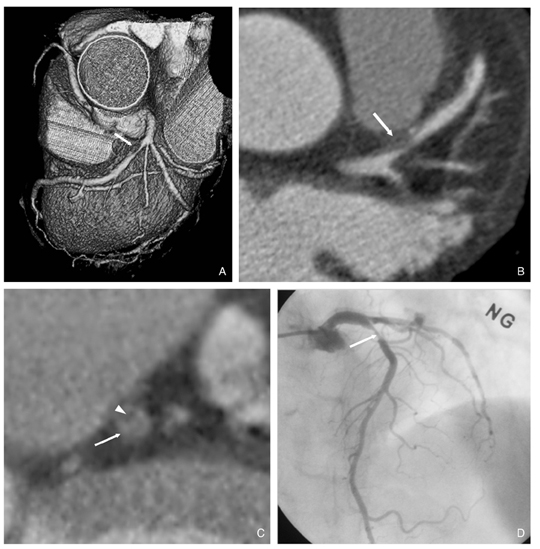
Figure 4 67-year-old female with chest pain. Volume-rendered (A) and axial reformatted (B) images show stenosis (arrow) in the proximal left anterior descending branch. Short-axial reformatted image (C) of the vessel shows significant stenosis (arrow) with eccentric lumen and lipid area (arrowhead). Catheter angiography (D) correlated well with CT angiography in visual grading of stenosis (arrow) of the coronary artery.
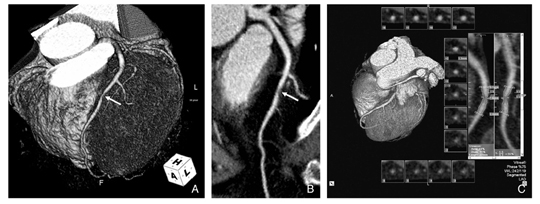
Figure 5 66-year-old female with chest pain. Volume-rendered (A) and maximum intensity projection (B) images show stenosis (arrow) in the mid left anterior descending branch. Semiautomatic quantitative approach (C) revealed a 55% stenosis.
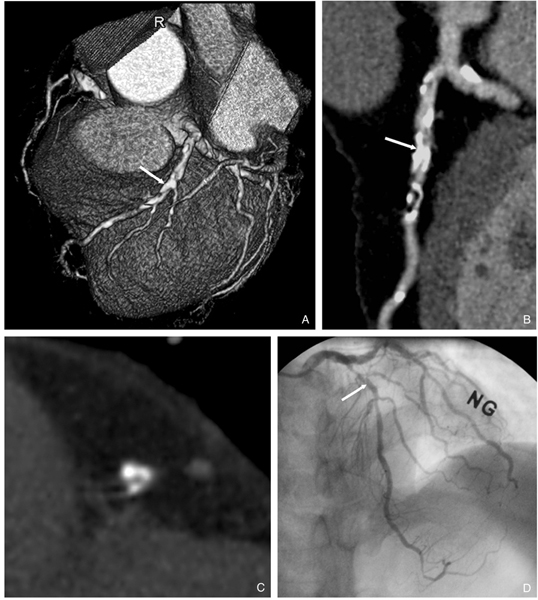
Figure 6 65-year-old male with previous myocardial infarction. There are multiple calcifications in proximal to mid left anterior descending branch. Volume-rendered (A) and maximum intensity projection (B) images show dense tubular calcifications (arrows) in mid left anterior descending branch adjacent to the origin of 1st diagonal branch. Short-axial image (C) shows an almost obscured lumen in that segment. However, catheter angiography reveals only mild stenosis in the same segment. This case illustrates an example of overestimation of the stenosis degree at CT angiography due to blooming artifact of calcium.
Reference
-
1. Naghavi M, Libby P, Falk E, Casscells SW, Litovsky S, Willerson JT, et al. From vulnerable plaque to vulnerable patient: a call for new definitions and risk assessment strategies: Part I. Circulation. 2003. 108:1664–1672.2. Choe YH. Noninvasive imaging of atherosclerotic plaques using MRI and CT. Korean Circulation J. 2005. 35:5–18.
Article3. Viles-Gonzalez JF, Poon M, Sanz J, Rius T, Nikolaou K, Fayad ZA, Fuster V, Badimon JJ. In vivo 16-slice, multidetector-row computed tomography for the assessment of experimental atherosclerosis: comparison with magnetic resonance imaging and histopathology. Circulation. 2004. 110:1467–1472.
Article4. Nikolaou K, Becker CR, Muders M, Babaryka G, Scheidler J, Flohr T, Loehrs U, Reiser MF, Fayad ZA. Multidetector-row computed tomography and magnetic resonance imaging of atherosclerotic lesions in human ex vivo coronary arteries. Atherosclerosis. 2004. 174:243–252.
Article5. Schroeder S, Kuettner A, Wojak T, Janzen J, Heuschmid M, Athanasiou T, Beck T, Burgstahler C, Herdeg C, Claussen CD, Kopp AF. Non-invasive evaluation of atherosclerosis with contrast enhanced 16 slice spiral computed tomography: results of ex vivo investigations. Heart. 2004. 90:1471–1475.
Article6. Becker CR, Nikolaou K, Muders M, Babaryka G, Crispin A, Schoepf UJ, Loehrs U, Reiser MF. Ex vivo coronary atherosclerotic plaque characterization with multi-detector-row CT. Eur Radiol. 2003. 13:2094–2098.
Article7. Schroeder S, Kopp AF, Baumbach A, Meisner C, Kuettner A, Georg C, Ohnesorge B, Herdeg C, Claussen CD, Karsch KR. Noninvasive detection and evaluation of atherosclerotic coronary plaques with multislice computed tomography. J Am Coll Cardiol. 2001. 37:1430–1435.
Article8. Kopp AF, Schroeder S, Baumbach A, Kuettner A, Georg C, Ohnesorge B, Heuschmid M, Kuzo R, Claussen CD. Non-invasive characterisation of coronary lesion morphology and composition by multislice CT: first results in comparison with intracoronary ultrasound. Eur Radiol. 2001. 11:1607–1611.
Article9. Leber AW, Knez A, Becker A, Becker C, von Ziegler F, Nikolaou K, Rist C, Reiser MF, White C, Steibeck G, Boekstegers P. Accuracy of multidetector spiral computed tomography in identifying and differentiating the composition of coronary atherosclerotic plaques: a comparative study with intracoronary ultrasound. J Am Coll Cardiol. 2004. 43:1241–1247.
Article10. Hoffmann U, Moselewski F, Nieman K, Jang I-K, Ferencik M, Rahman AM, Cury RC, Abbara S, Joneidi-Jafari H, Achenbach S, Brady TJ. Noninvasive assessment of plaque morphology and composition in culprit and stable lesions in acute coronary syndrome and stable lesions in stable angina by multidetector computed tomography. J Am Coll Cardiol. 2006. 47:1655–1662.
Article11. Leschka S, Wildermuth S, Boehm T, Desbiolles L, Husmann L, Plass A, Koepfli P, Schepis T, Marincek B, Kaufmann PA, Alkadhi H. Noninvasive Coronary Angiography with 64-Section CT: Effect of average heart rate and heart rate variability on image quality. Radiology. 2006. 241:378–385.
Article12. Cury RC, Pomerantsev EV, Ferencik M, Hoffmann U, Nieman K, Meselewski F, Abbara S, Jang I-K, Brady TJ, Achenbach S. Comparison of the degree of coronary stenosis by multidetector computed tomography versus by quantitative coronary angiography. Am J Cardiol. 2005. 96:784–787.
Article13. Leber AW, Knez A, von Ziegler F, Becker A, Nokolaou K, Paul S, Wintersperger B, Reiser M, Becker CR, Steinbeck G, Boekstegers P. Quantification of obstructive and nonobstructive coronary lesions by 64-slice computed tomography. A comparative study with quantitative coronary angiography and intravascular ultrasound. J Am Coll Cardiol. 2005. 46:147–154.
Article14. Caussin C, Larchez C, Ghostine S, Pesenti-Rossi D, Daoud B, Habis M, Sigal-Cinqualbre A, Perrier E, Angel CY, Lancelin B, Paul JF. Comparison of coronary minimal lumen area quantification by sixty-four-slice computed tomography versus intravascular ultrasound for intermediate stenosis. Am J Cardiol. 2006. 98:871–876.
Article15. Busch S, Johnson TR, Nikolaou K, von Ziegler F, Knez A, Reiser MF, Becker CR. Visual and automatic grading of coronary artery stenoses with 64-slice CT angiography in reference to invasive angiography. Eur Radiol. 2006. 12. 16. [Epub ahead of print].
Article16. Khan MF, Wesarg S, Gurung J, Dogan S, Maataoui A, Brehmer B, Herzog C, Ackermann H, Assmus B, Vogl TJ. Facilitating coronary artery evaluation in MDCT using a 3D automatic vessel segmentation tool. Eur Radiol. 2006. 16:1789–1795.
Article17. Marquering HA, Dijkstra J, de Koning PJH, Stoel BC, Reiber JHC. Towards quantitative analysis of coronary CTA. Int J Cardiovasc Imaging. 2005. 21:73–84.
Article18. van der Zaag-Loonen HJ, Dikkers R, De Bock GH, Oudkerk M. The clinical value of a negative multi-detector computed tomographic angiography in patients with suspected coronary disease: a meta analysis. Eur Radiol. 2006. 16:2748–2756.
Article19. Garcia MJ, Lessick J, Hoffmann MHK. CATSCAN Study Investigators. Accuracy of 16-row multidetector computed tomography for the assessment of coronary artery stenosis. JAMA. 2006. 296:403–411.
Article20. Raff GL, Gallagher MJ, O'Neill WW, Goldstein JA. Diagnostic accuracy of noninvasive coronary angiography using 64-slice spiral computed tomography. J Am Coll Cardiol. 2005. 46:552–557.
Article21. Ghostine S, Caussin C, Daoud B, Habis M, Perrier E, Pesenti-Rossi D, Sigal-Cinqualbre A, Angel CY, Lancelin B, Capderou A, Paul JF. Non-invasive detection of coronary artery disease in patients with left bundle branch block using 64-slice computed tomography. J Am Coll Cardiol. 2006. 48:1929–1934.
Article22. Nikolaou K, Knez A, Rist C, Wintersperger BJ, Leber A, Johnson T, Reiser MF, Becker CR. Accuracy of 64-MDCT in the diagnosis of ischemic heart disease. Am J Roentgenol. 2006. 187:111–117.
Article23. Ehara M, Surmely J-F, Kawai M, Katoh O, Matsubara T, Terashima M, Tsuchikane E, Kinoshita Y, Suzuki T, Ito T, Takeda Y, Nasu K, Tanaka N, Murata A, Suzuki Y, Sato K, Suzuki T. Diagnostic accuracy of 64-slice computed tomography for detecting angiographically significant coronary artery stenosis in an unselected consecutive patient population: comparison with conventional invasive angiography. Circulation J. 2006. 70:564–571.
Article24. Fine JJ, Hopkins CB, Ruff N, Newton FC. Comparison of accuracy of 64-slice cardiovascular computed tomography with coronary angiography in patients with suspected coronary disease. Am J Cardiol. 2006. 97:173–174.
Article25. Leschka S, Alkadhi H, Plass A, Desbiolles L, Grunenfelder J, Marincek B, Wildermuth S. Accuracy of MSCT coronary angiography with 64-slice technology: first experience. Eur Heart J. 2005. 26:1482–1487.
Article26. Mollet NR, Cademartiri F, van Mieghem CA, Runza G, McFadden EP, Baks T, Serruys PW, Krestin GP, de Feyter PJ. High-resolution spiral computed tomography coronary angiography in patients referred for diagnostic conventional coronary angiography. Circulation. 2005. 112:2318–2323.
Article27. Pugliese F, Mollet NR, Runza G, van Mieghem C, Meijboom WB, Malagutti P, Baks T, Krestin GP, deFeyter PJ, Cademartiri F. Diagnostic accuracy of non-invasive 64-slice CT coronary angiography in patients with stable angina pectoris. Eur Radiol. 2006. 16:575–582.
Article28. Ropers D, Rixe J, Anders K, Kuttner A, Baum U, Bautz W, Daniel WG, Achenbach S. Usefulness of multidetector row computed tomography with 64- × 0.6-mm collimation and 330-ms rotation for the noninvasive detection of significant coronary artery stenoses. Am J Cardiol. 2006. 97:343–348.
Article29. Scheffel H, Alkadhi H, Plass A, Vachenauer R, Desbiolles L, Gaemperli O, Schepis T, Frauenfelder T, Schertler T, Husmann L, Grunenfelder J, Genoni M, Kaufmann PA, Marincek B, Leschka S. Accuracy of dual-source CT coronary angiography: first experience in a high pre-test probability population without heart rate control. Eur Radiol. 2006. 16:2739–2747.
Article30. Sakuma H, Ichikawa Y, Chino S, Hirano T, Makino K, Takeda K. Detection of coronary artery stenosis with whole-heart coronary magnetic resonance angiography. J Am Coll Cardiol. 2006. 48:1946–1950.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Noninvasive Imaging of Atherosclerotic Plaques Using MRI and CT
- An Overview of Myocardial Bridging With a Focus on Multidetector CT Coronary Angiographic Findings
- Coronary CT Angiography
- Evaluation of Atherosclerotic Plaque in Patients without Coronary Artery Calcification Using Multidetector Row Computed Tomography: A Preliminary Report of 110 patients
- Plaque Characteristics on Coronary CT Angiography: Effects on the Degree of Coronary Artery Stenosis
