Exophytic Benign and Malignant Hepatic Tumors: CT Imaging Features
- Affiliations
-
- 1Department of Radiology, Kyung Hee University Medical Center, Seoul, Korea. radhjkim@khu.ac.kr
- 2Department of Radiology, University of Ulsan College of Medicine and Asan Medical Center, Seoul, Korea.
- KMID: 1734277
- DOI: http://doi.org/10.3348/kjr.2008.9.1.67
Abstract
- Our objective is to describe the CT features of exophytic hepatic tumors those may pose a diagnostic challenge because of the uncertainty of tumor origin. The beak sign and the feeding artery of a tumor are useful diagnostic indicators of exophytic hepatic tumors. Two- or three-dimensional reformation images are also helpful for diagnosis. The CT features of exophytic hepatic tumors are similar to those of the usual intrahepatic tumors except for their location.
Keyword
MeSH Terms
Figure
-
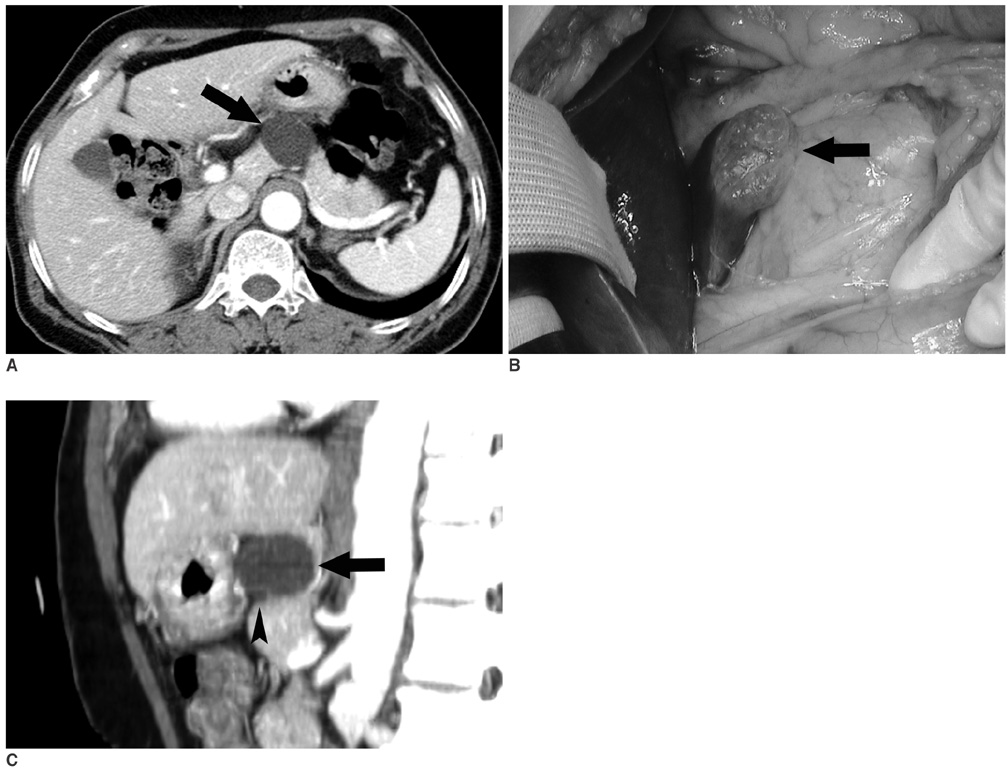
Fig. 1 A 64-year-old woman with an exophytic hepatic cyst. A. A contrast-enhanced CT scan shows a well-defined, cystic mass (arrow) in the pancreas. Mural nodule or septation is not noted. The lesion was initially interpreted as a mucinous cystic neoplasm of the pancreas. B. A photograph taken during surgery shows a cyst (arrow) arising from the caudate lobe. C. A sagittal reformation image shows a cyst with beak sign (arrow) in its contact surface with the caudate lobe; however, this cyst shows a dull edge (arrowhead) in its contact surface with the pancreas.
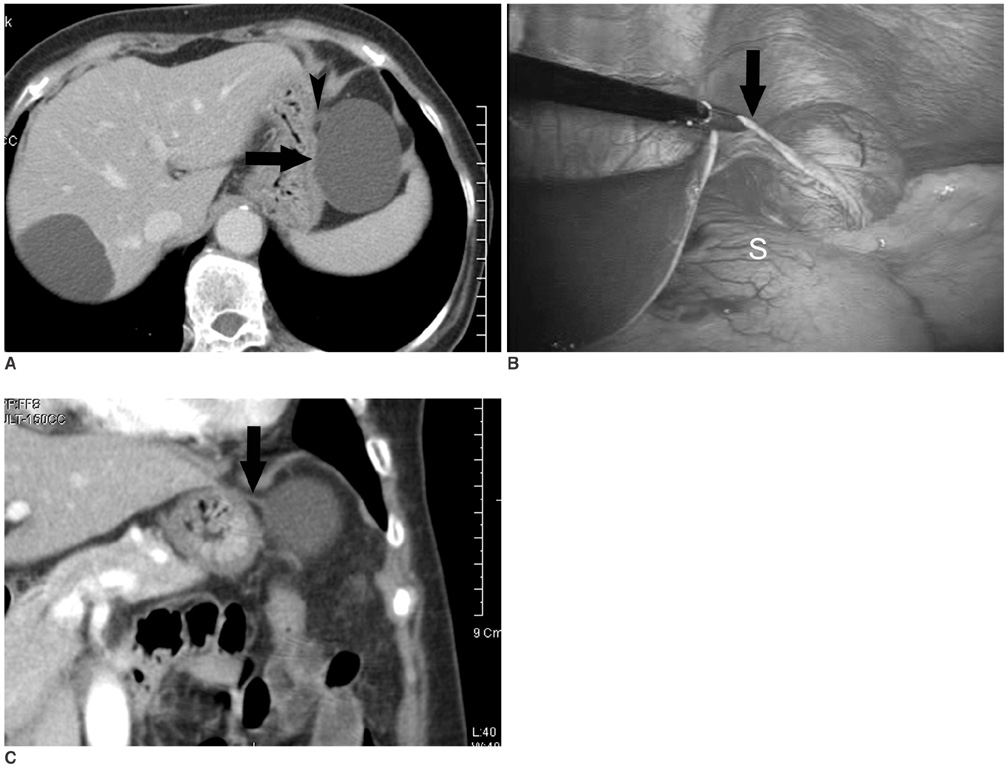
Fig. 2 A 72-year-old woman with an exophytic hepatic cyst. A. A contrast-enhanced CT scan shows a well-defined, cystic mass (arrow) adjacent to the greater curvature side of the stomach. Initially, the lesion was interpreted as an omental cyst, lymphangioma, or duplication cyst. Thin band-like opacity (arrowhead) is suspicious at the anteromedial aspect of the cystic mass. B. A photograph taken during surgery shows a thin stalk (arrow) that connects the cyst with the lateral segment, crossing over the stomach (S). C. A coronal reformation image shows a thin stalk (arrow) connecting the cyst with the lateral segment.
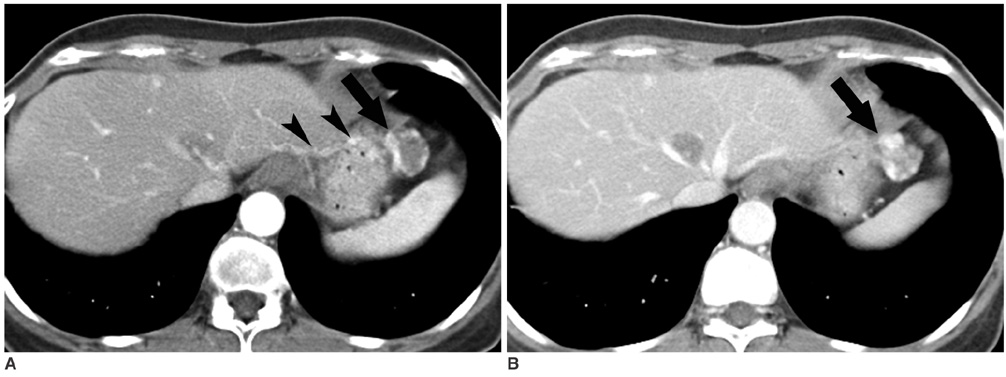
Fig. 3 A 53-year-old woman with a pedunculated hemangioma. A. A contrast-enhanced CT scan during hepatic arterial phase shows a small nodular lesion (arrow) adjacent to the greater curvature side of the stomach. There is a vascular pedicle (arrowheads) connecting nodule with the lateral segment (prominent feeding artery sign). It shows dense peripheral enhancement. B. A contrast-enhanced CT scan during portal venous phase shows centripetal enhancement of this small nodule (arrow).
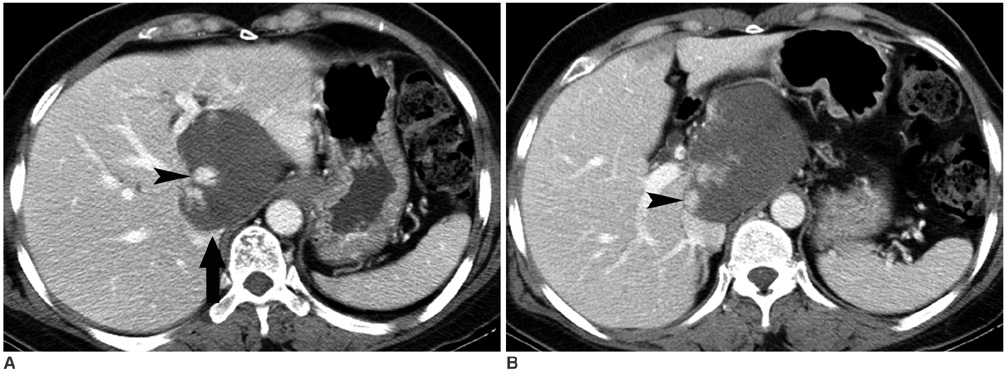
Fig. 4 A 51-year-old woman with an exophytic hemangioma. A, B. Contrast-enhanced CT scans show a large low density mass in the lesser sac. The beak sign is seen in its contact surface with the caudate lobe (arrow in A) and dense peripheral globular enhancement (arrowheads) is noted. A Tc-99m RBC scan (not shown) shows a blood pooling mass in the same location as on the CT image.
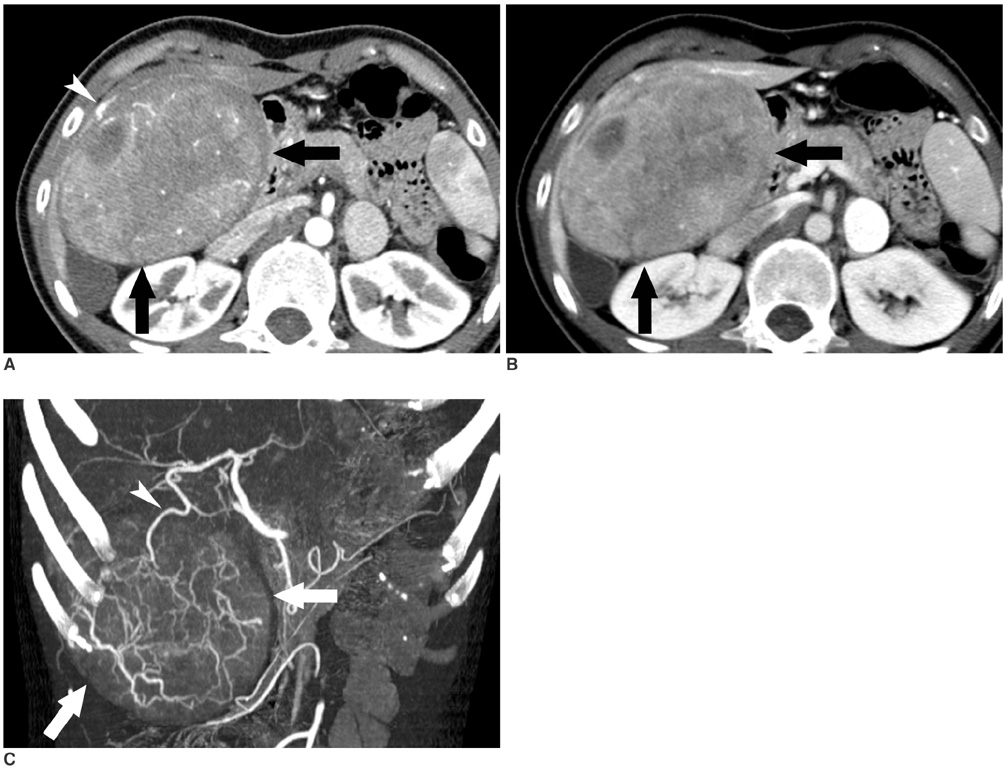
Fig. 5 A 23-year-old woman with an exophytic hepatocelluar adenoma. A. A contrast-enhanced CT scan during hepatic arterial phase shows a heterogeneous and mild high-density mass (arrows), below the right lobe. Prominent subcapsular vessels are noted (arrowhead). The beak sign is not definite on serial axial images (not shown). B. On a contrast-enhanced CT scan during portal venous phase, the mass (arrows) shows persistent heterogeneity and a slightly decreased density. C. An oblique coronal maximum-intensity-projection image during hepatic arterial phase shows a large branch (arrowhead) from the right hepatic artery supplying this mass (arrows).
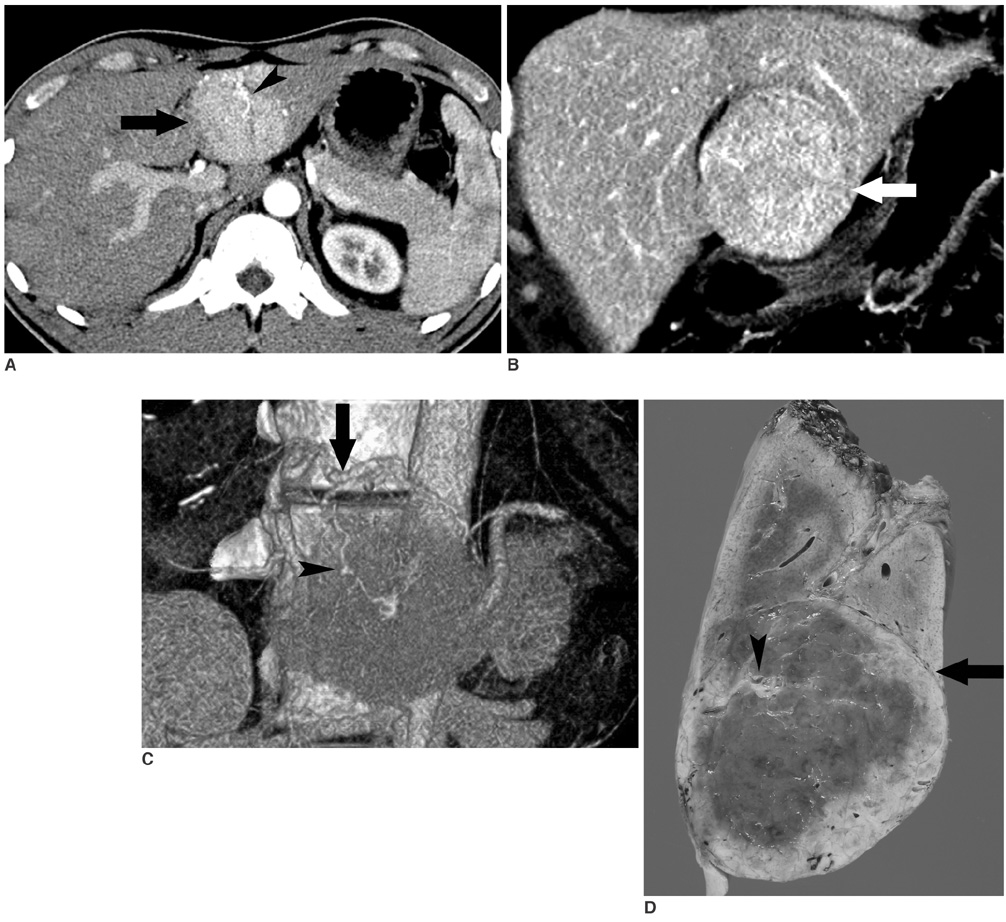
Fig. 6 A 26-year-old man with an exophytic focal nodular hyperplasia. A. A contrast-enhanced CT scan during hepatic arterial phase shows a homogeneous high-density mass (arrow) in the left lobe. The feeding artery (arrowhead) is noted in the central portion of the mass. B. On a coronal reformation image during the portal venous phase, the beak sign is noted in its contact surface with the lateral segment (arrow). C. An oblique coronal volume rendering image during hepatic arterial phase shows a prominent left hepatic artery (arrow) and a small central artery (arrowhead) supplying this mass. D. A pathological specimen shows the beak sign (arrow) in its contact surface with the lateral segment and a small central artery (arrowhead) within the fibrous scar.

Fig. 7 A 52-year-old woman with an exophytic angiomyolipoma. A. A contrast-enhanced CT scan during hepatic arterial phase shows a fatty mass in the lateral segment of the liver. This fatty mass shows the beak sign (arrow) in its contact surface with the lateral segment. The left hepatic artery (arrowhead) is enlarged and it is a prominent feeding artery supplying this fatty mass. B. On a contrast-enhanced CT scan during portal venous phase, 4 cm below (A), most of the huge fatty mass (arrows) is located in the peritoneal cavity. C. Hepatic arteriography shows a dilated left hepatic artery (arrow) and prominent tumor vessels.
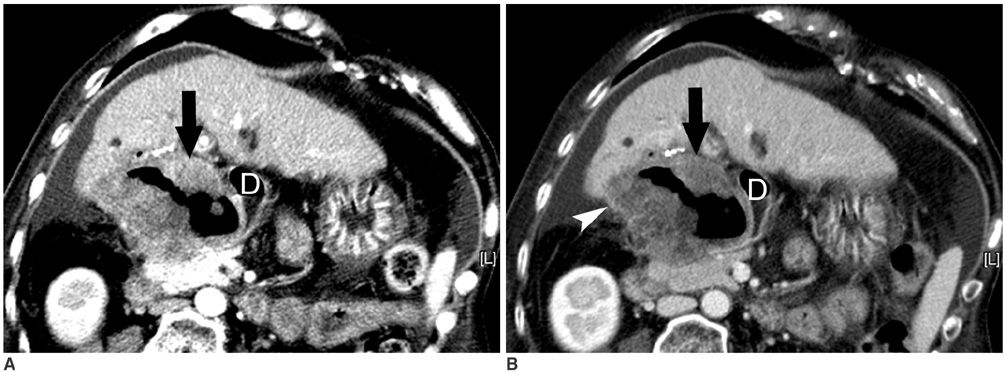
Fig. 8 A 57-year-old woman with an exophytic hepatocellular carcinoma with duodenal invasion. A. A contrast-enhanced CT scan during hepatic arterial phase shows a large necrotic mass, compressing the lateral wall of the duodenum (D). The solid portion of this mass (arrow) shows iso-density in comparison with the liver parenchyma. On a contrast-enhanced CT scan during portal venous phase, the solid portion of this mass (arrow) shows low density in comparison with the liver parenchyma. The beak sign (arrowhead) is noted in its contact surface with the right lobe. The fine nodular hepatic surface suggests liver cirrhosis. The lateral wall of the duodenum (D) is not definite.

Fig. 9 A 57-year-old man with an exophytic hepatocellular carcinoma and bile duct invasion. A. A contrast-enhanced CT scan during hepatic arterial phase shows a small high-density mass (arrow) posterior to the lateral segment. Dense tubular enhancement (arrowhead) in the lateral segment shows a connection with this small mass. B. On a contrast-enhanced CT scan during portal venous phase, the small mass (arrow) and tubular lesion (arrowhead) shows low density in comparison with liver parenchyma. A fine nodular hepatic surface and hypertrophied lateral segment suggest liver cirrhosis. C. On endoscopic retrograde cholangiography, there is a filling defect (arrow) in the B2 duct, which was seen as a tubular high density on hepatic arterial phase image (A). On surgery, it was confirmed as an exophytic hepatocellular carcinoma and bile duct invasion.

Fig. 10 A 66-year-old woman with an exophytic cholangiocellular carcinoma. A. A contrast-enhanced CT scan during hepatic arterial phase shows a large mass with heterogeneous peripheral enhancement in the left lateral segment. It shows the beak sign (arrow) in its contact surface with the lateral segment. B. A contrast-enhanced CT scan during portal venous phase shows centripetal progression of contrast enhancement (arrowheads) of this exophytic mass (arrow). On surgery, the lesion was confirmed as an exophytic cholangiocellular carcinoma.

Fig. 11 A 44-year-old man with exophytic hepatic metastasis from rectal cancer. A contrast-enhanced CT scan shows multiple low density masses in the liver of a patient with rectal cancer (not shown). A low density mass is seen adjacent to the lateral segment. The beak sign (arrow) is noted in its contact surface with the lateral segment.
Cited by 1 articles
-
Giant pedunculated hepatocellular carcinoma masquerading as a pelvic mass: a case report
Hae Il Jung
Korean J Hepatobiliary Pancreat Surg. 2014;18(2):56-59. doi: 10.14701/kjhbps.2014.18.2.56.
Reference
-
1. Bader TR, Braga L, Semelka RC. Exophytic benign tumors of the liver: appearance on MRI. Magn Reson Imaging. 2001. 19:623–628.2. Nishino M, Hayakawa K, Minami M, Yamamoto A, Ueda H, Takasu K. Primary retroperitoneal neoplasms: CT and MR imaging findings with anatomic and pathologic diagnostic clues. Radiographics. 2003. 23:45–57.3. Murphy BJ, Casillas J, Ros PR, Morillo G, Albores-Saavedra J, Rolfes DB. The CT appearance of cystic masses of the liver. Radiographics. 1989. 9:307–322.4. Quinn SF, Benjamin GG. Hepatic cavernous hemangiomas: simple diagnostic sign with dynamic bolus CT. Radiology. 1992. 182:545–548.5. Brancatelli G, Federle MP, Blachar A, Grazioli L. Hemangioma in the cirrhotic liver: diagnosis and natural history. Radiology. 2001. 219:69–74.6. Vilgrain V, Boulos L, Vullierme MP, Denys A, Terris B, Menu Y. Imaging of atypical hemangiomas of the liver with pathologic correlation. Radiographics. 2000. 20:379–397.7. Brancatelli G, Federle MP, Vullierme MP, Lagalla R, Midiri M, Vilgrain V. CT and MR imaging evaluation of hepatic adenoma. J Comput Assist Tomogr. 2006. 30:745–750.8. Ichikawa T, Federle MP, Grazioli L, Nalesnik M. Hepatocellular adenoma: multiphasic CT and histopathologic findings in 25 patients. Radiology. 2000. 214:861–868.9. Goldstein HM, Neiman HL, Mena E, Bookstein JJ, Appelman HD. Angiographic findings in benign liver cell tumors. Radiology. 1974. 110:339–343.10. Brancatelli G, Federle MP, Grazioli L, Blachar A, Peterson MS, Thaete L. Focal nodular hyperplasia: CT findings with emphasis on multiphasic helical CT in 78 patients. Radiology. 2001. 219:61–68.11. Akatsu T, Sakamoto M, Shimazu M, Kitajima M. Pedunculated angiomyolipoma of the liver with a predominant pelioid pattern. Virchows Arch. 2004. 444:467–469.12. Bret PM, Bretagnolle M, Gaillard D, Plauchu H, Labadie M, Lapray JF, et al. Small, asymptomatic angiomyolipomas of the kidney. Radiology. 1985. 154:7–10.13. Valls C, Iannacconne R, Alba E, Murakami T, Hori M, Passariello R, et al. Fat in the liver: diagnosis and characterization. Eur Radiol. 2006. 16:2292–2308.14. Yeh CN, Lee WC, Jeng LB, Chen MF. Pedunculated hepatocellular carcinoma: clinicopathologic study of 18 surgically resected cases. World J Surg. 2002. 26:1133–1138.15. Horie Y, Katoh S, Yoshida H, Imaoka T, Suou T, Hirayama C. Pedunculated hepatocellular carcinoma. Report of three cases and review of literature. Cancer. 1983. 51:746–775.16. Kim KW, Auh YH, Chi HS, Lee SI. CT of retroperitoneal extension of hepatoma mimicking adrenal tumor. J Comput Assist Tomogr. 1993. 17:599–602.17. Jung AY, Lee JM, Choi SH, Kim SH, Lee JY, Kim SW, et al. CT features of an intraductal polypoid mass: differentiation between hepatocellular carcinoma with bile duct tumor invasion and intraductal papillary cholangiocarcinoma. J Comput Assist Tomogr. 2006. 30:173–181.18. Ros PR, Buck JL, Goodman ZD, Ros AM, Olmsted WW. Intrahepatic cholangiocarcinoma: radiologic-pathologic correlation. Radiology. 1988. 167:689–693.19. Valls C, Guma A, Puig I, Sanchez A, Andia E, Serrano T, et al. Intrahepatic peripheral cholangiocarcinoma: CT evaluation. Abdom Imaging. 2000. 25:490–496.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Hepatocellular Adenoma and Focal Nodular Hyperplasia
- Penetration of Hepatic Veins Through the Hepatic Neoplasms : Report of Three Cases
- MRI Findings and Differential Diagnosis of Benign and Malignant Tumors of the Uterine Corpus
- Vascular tumors of the liver: A brief review
- Solitary Pulmonary Nodule: CT Findings
