A Case of Primary Extragastrointestinal Stromal Tumor Presenting as Peritoneal Dissemination
- Affiliations
-
- 1Department of Internal Medicine, The Catholic University of Korea College of Medicine, Seoul, Korea. drkimtaeho@yahoo.co.kr
- 2Department of Pathology, The Catholic University of Korea College of Medicine, Seoul, Korea.
- KMID: 1718374
- DOI: http://doi.org/10.4166/kjg.2010.56.5.319
Abstract
- Gastrointestinal stromal tumor (GIST) is the most common mesenchymal tumor of the gastrointestinal tract, but also occurs at a lower frequency in extra-gastrointestinal regions such as omentum, mesentery, retroperitoneum and undefined abdominal sites. This tumor is called extragastrointestinal stromal tumor (EGIST). EGIST is mostly diagnosed as a cystic mass, but rarely occurs as a disseminated abdominal tumor. We experienced a 70-year-old man with primary EGIST presenting as peritoneal dissemination. Abdominal CT showed diffuse peritoneal thickening with a large amount of ascites, but no definite mass lesion. Laparoscopic biopsy was performed and histologic findings showed tumor composed of epithelioid cells. In the results of immunohistochemical stains, the tumor showed positive reactivity with CD117 (c-kit), CD34, vimentin and actin, but negative reactivity with desmin and S-100 protein. On account of unresectability and histologic parameters of malignant behavior, he was started on imatinib.
MeSH Terms
Figure
-

Fig. 1. Abdominal CT finding. Diffuse peritoneal wall thickening was noted with a large amount of ascites. This finding was prominent in the greater omentum.

Fig. 2. Small bowel series and PET-CT findings. (A) Small bowel series showed a normal contour without evidence of extrinsic compression. (B) Diffuse FDG uptake along the peritoneal surface was noted. This finding was consistent with peritoneal carcinomatosis.

Fig. 3. Laparoscopic finding. Multiple tumor nodules were scat-tered on the peritoneal surface.
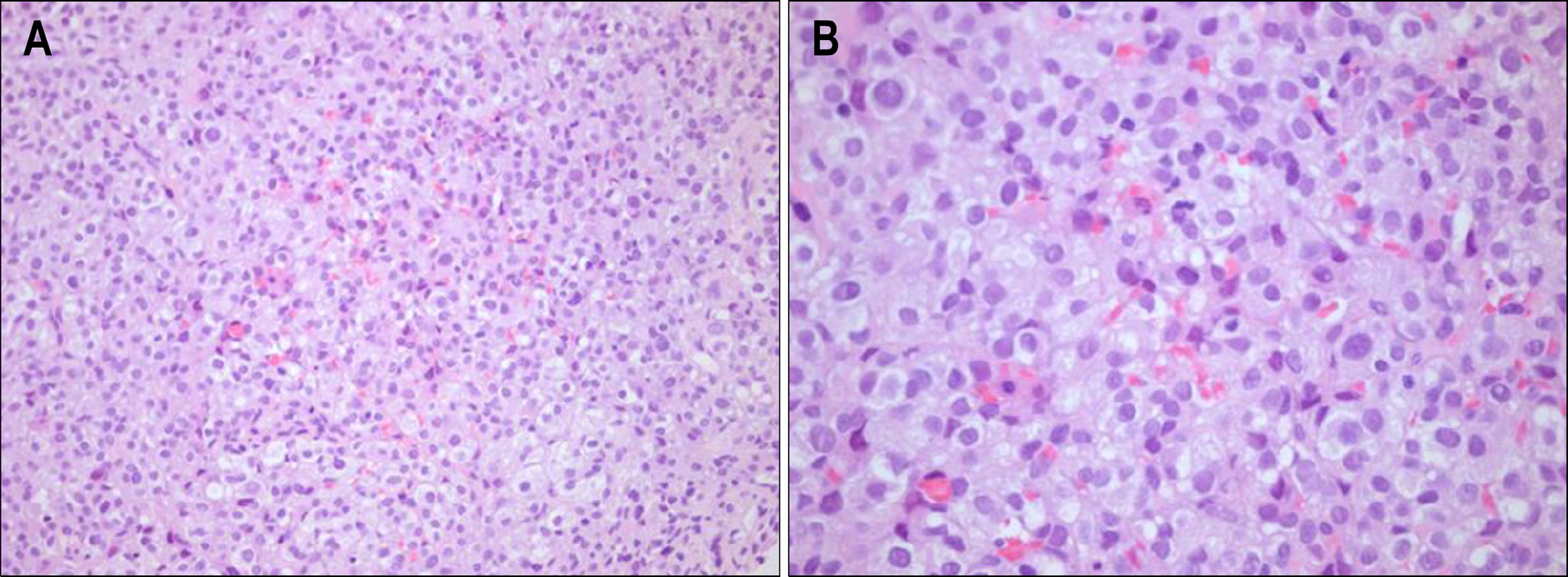
Fig. 4. Microscopic findings. (A) The tumor was composed of epithelioid cells (H&E stain, ×100). (B) The tumor cells showed high cel-lularity, but no necrosis (H&E stain, ×400).
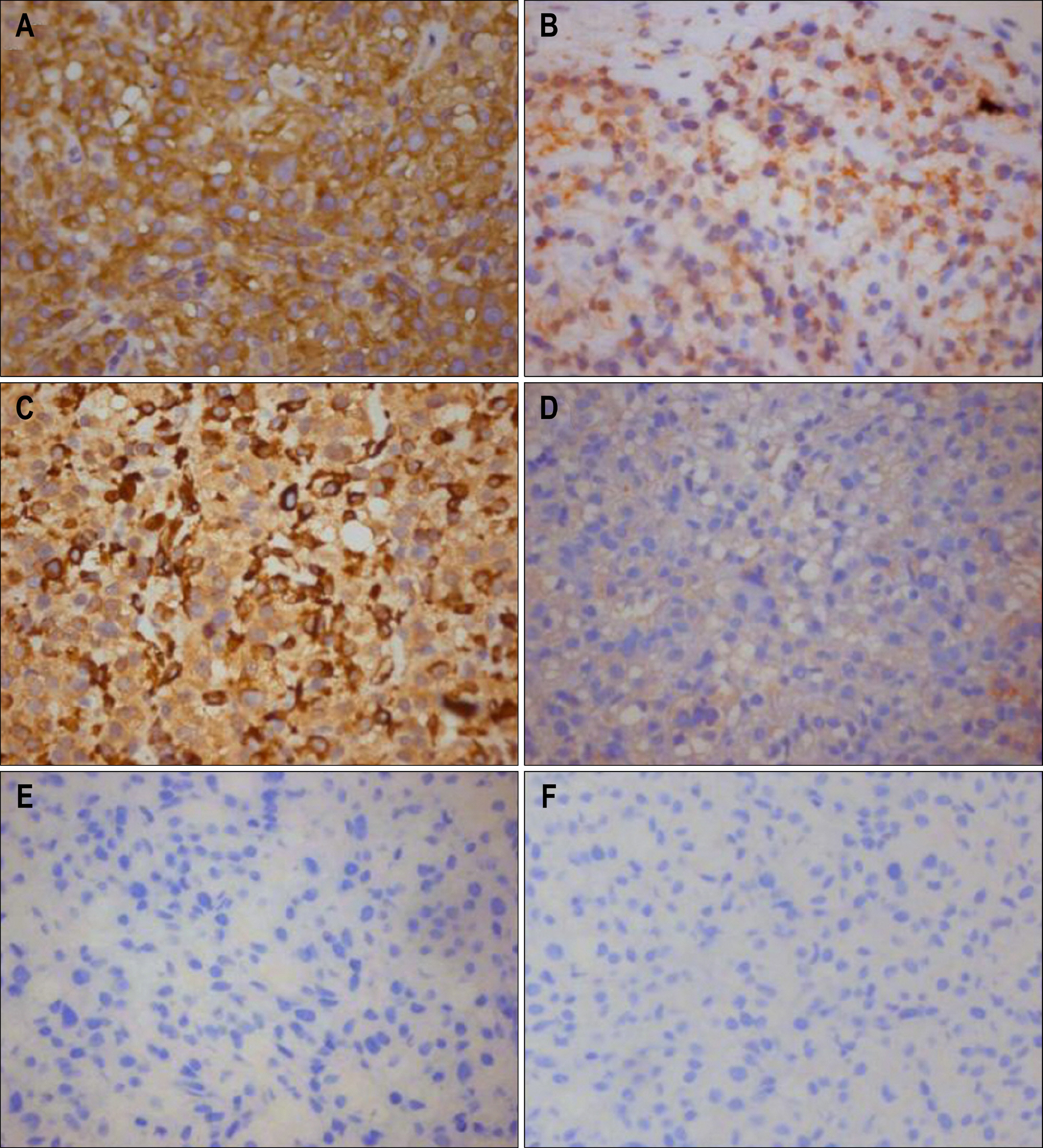
Fig. 5. Immunohistochemical findings. Tumor cells were positive for CD117(c-kit) (A), CD34 (B), vimentin (C), and actin (D). However, tumor cells were negative for desmin (E) and S-100 protein (F) (×200).
Reference
-
1. Choi KU, Kim JY, Park DY, et al. Primary extragastrointestinal stromal tumor (EGIST) of the greater omentum. Korean J Pathol. 2001; 35:347–350.2. Ko ES, Bae K, Jeon KN, et al. Extragastrointestinal stromal tumor presenting a large multilocular cystic mass arising from the greater omentum: a case report. J Korean Radiol Soc. 2004; 51:533–536.
Article3. Hwang KT, Chung JK, Jung IM, et al. Primary retroperitoneal malignant gastrointestinal stromal tumor mimicking adrenal mass. J Korean Surg Soc. 2009; 77:357–361.
Article4. Mazur MT, Clark HB. Gastric stromal tumors. Reappraisal of histogenesis. Am J Surg Pathol. 1983; 7:507–519.
Article5. Kindblom LG, Remotti HE, Aldenborg F, Meis-Kindblom JM. Gastrointestinal pacemaker cell tumor (GIPACT): gastrointestinal stromal tumors show phenotypic characteristics of the interstitial cells of Cajal. Am J Pathol. 1998; 152:1259–1269.6. Sircar K, Hewlett BR, Huizinga JD, Chorneyko K, Berezin I, Riddell RH. Interstitial cells of Cajal as precursors of gastrointestinal stromal tumors. Am J Surg Pathol. 1999; 23:377–389.
Article7. Fletcher CD, Berman JJ, Corless C, et al. Diagnosis of gastrointestinal stromal tumors: A consensus approach. Hum Pathol. 2002; 33:459–465.
Article8. Reith JD, Goldblum JR, Lyles RH, Weiss SW. Extragastrointestinal (soft tissue) stromal tumors: an analysis of 48 cases with emphasis on histologic predictors of outcome. Mod Pathol. 2000; 13:577–585.
Article9. Takahashi T, Kuwao S, Yanagihara M, Kakita A. A primary solitary tumor of the lesser omentum with immunohistochemical features of gastrointestinal stromal tumors. Am J Gastroenterol. 1998; 93:2269–2273.
Article10. Sakurai S, Hishima T, Takazawa Y, et al. Gastrointestinal stromal tumors and KIT-positive mesenchymal cells in the omentum. Pathol Int. 2001; 51:524–531.
Article11. Miettinen M, Monihan JM, Sarlomo-Rikala M, et al. Gastrointestinal stromal tumors/smooth muscle tumors (GISTs) primary in the omentum and mesentery: clinicopathologic and immunohistochemical study of 26 cases. Am J Surg Pathol. 1999; 23:1109–1118.12. Miettinen M, Sobin LH, Lasota J. Gastrointestinal stromal tumors presenting as omental masses–a clinicopathologic analysis of 95 cases. Am J Surg Pathol. 2009; 33:1267–1275.
Article13. Miettinen M, Lasota J. Gastrointestinal stromal tumors: review on morphology, molecular pathology, prognosis, and differential diagnosis. Arch Pathol Lab Med. 2006; 130:1466–1478.
Article14. Liegl-Atzwanger B, Fletcher JA, Fletcher CD. Gastrointestinal stromal tumors. Virchows Arch. 2010; 456:111–127.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Extra-gastrointestinal Stromal Tumor on the Inner Urinary Bladder Wall
- A Case of an Extragastrointestinal Stromal Tumor of the Pelvic Cavity Presenting with Hematuria
- Extragastrointestinal Stromal Tumor Mimicking Gastric Subepithelial Tumor
- Primary Extragastrointestinal Stromal Tumor of Retroperitoneum: Poor Response to Tyrosine Kinase Inhibitor
- An Extragastrointestinal Stromal Tumor in the Omentum With Peritoneal Seeding Mimicking an Appendiceal Mucinous Cancer With Carcinomatosis
