A Case of Hepatic Congestion Due to Right Heart Failure Mimicking Liver Tumor
- Affiliations
-
- 1Department of Internal Medicine, Yonsei Liver Cancer Special Clinic, Yonsei University College of Medicine, Seoul, Korea. dyk1025@yuhs.ac
- KMID: 1718364
- DOI: http://doi.org/10.4166/kjg.2010.56.4.264
Abstract
- This report describes a patient with hepatic congestion due to right heart failure mimicking liver tumor. The patient had a history of breast cancer and left total mastectomy 30 years ago, tricuspid valve regurgitation and tricuspid valve replacement 4 years ago. Three years ago, abdominal contrast-enhanced computed tomography (CT) was performed to evaluate inguinal hernia, which revealed multiple small hepatic nodules. After 1 year, the number and size of liver nodules were increased in CT scan. The patient underwent gun biopsy and histopathology revealed sinusoid enlargement. The patient recently had jaundice, abdominal distension, and peripheral edema. Liver dynamic CT scan was done to evaluate the palpable liver. The number and size of liver nodules were more increased in CT than 2 years ago. In magnetic resonance imaging (MRI), numerous variable sized ill-defined nodules replacing entire liver with progressing centripetal enhancement, which were suggestive of malignancy such as angiosarcoma, were noted. MRI finding suspects malignancy or hemangiosarcoma. Finally, the patient received repeated gun biopsy, and histopathology revealed findings compatible with hepatic congestion.
MeSH Terms
Figure
-
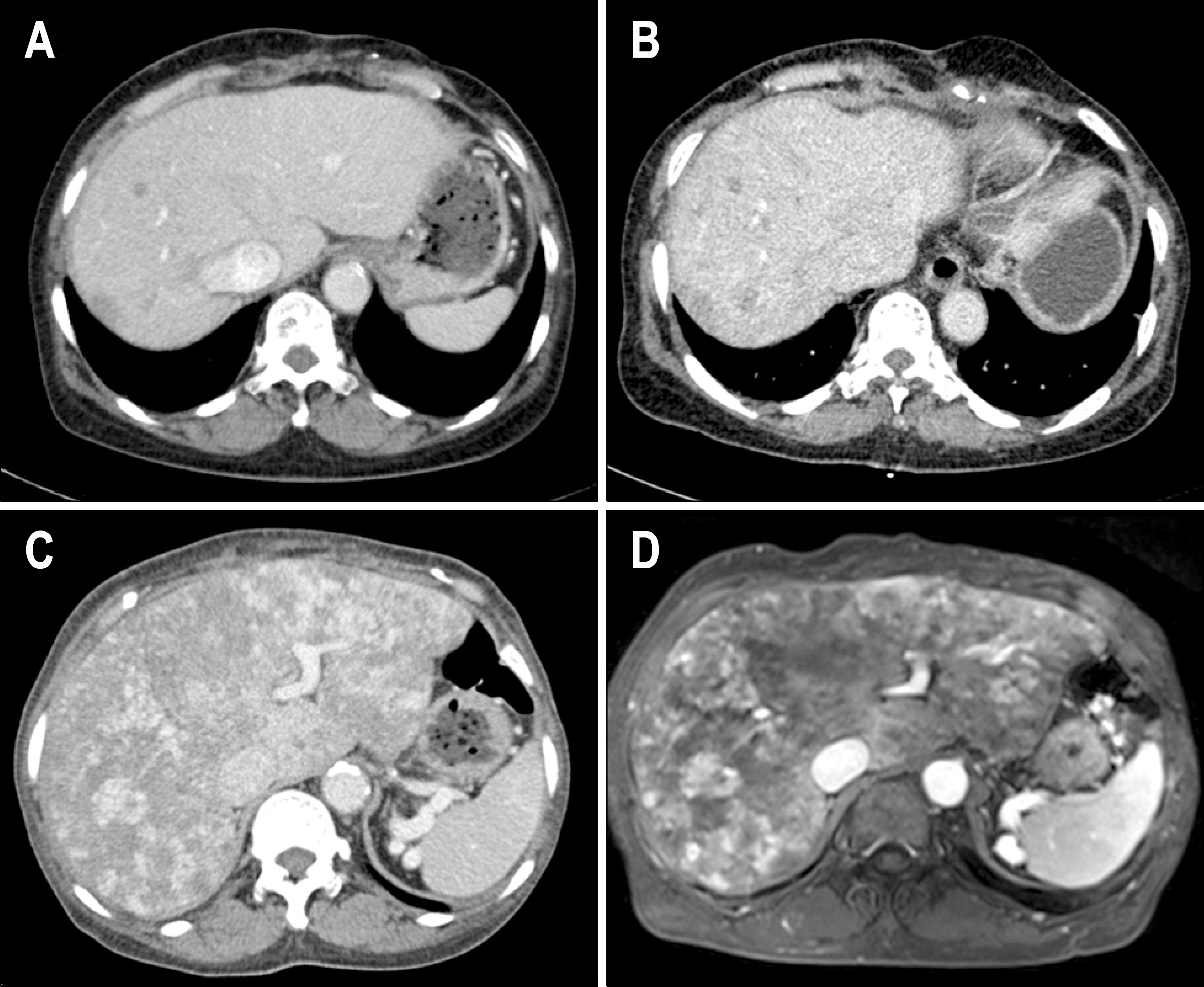
Fig. 1. (A) Three years ago, CT showed multiple, variable sized, and ill-defined low density nodule scattering through entire liver. (B) Two years ago, CT showed variable sized and ill-defined low density nodule increased in size and number. (C) At this time, CT showed previously noted low density nodules in both lobes of the liver increased in size and number and dilated IVC and hepatic veins, inhomogenous enhancement of hepatic parenchyma. (D) In T2 weighted MRI scan, numerous nodules replaced entire liver with progressing centripetal enhancement.

Fig. 2. (A) Initial liver specimen showed sinusoidal dilatation and fibrous septal containing ductular proliferation and abnormal vessel (H&E, ×200). (B) Following liver specimen showed marked sinusoidal dilatation with focal sinusoidal fibrin thrombi, portal fibrosis and focal ductular proliferation (H&E, ×100).
Reference
-
1. Kiernan F. The anatomy and physiology of the liver. Phil Trans R Soc Lond. 1833; 123:711–770.2. Mallory FB. Chronic passive congestion of the liver. J Med Res. 1911; 24:455–462.3. Holley HC, Koslin DB, Berland LL, Stanley RJ. Inhomogen-eous enhancement of liver parenchyma secondary to passive congestion: contrast-enhanced CT. Radiology. 1989; 170:795–800.
Article4. Nyman R, Kagevi I. Budd-Chiari syndrome misinterpreted as an infiltrating liver mass. A case report. Acta Radiol. 1995; 36:393–395.5. Jang HJ, Lee WJ, Lee SJ, Kim SH, Lim HK, Lim JH. Focal eosinophilic necrosis of the liver in patients with underlying gastric or colorectal cancer: CT differentiation from metastasis. Korean J Radiol. 2002; 3:240–244.
Article6. Rosen PR, Groshen S, Saigo PE, Kinne DW, Hellman S. A longterm follow-up study of survival in stage I (T1N0M0) and stage II (T1N1M0) breast carcinoma. J Clin Oncol. 1989; 7:355–366.
Article7. Marty M, Cognetti F, Maraninchi D, et al. Randomized phase II trial of the efficacy and safety of trastuzumab combined with docetaxel in patients with human epidermal growth factor receptor 2-positive metastatic breast cancer administered as first-line treatment: the M77001 study group. J Clin Oncol. 2005; 23:4265–4274.
Article8. Chan S, Friedrichs K, Noel D, et al. Prospective randomized trial of docetaxel versus doxorubicin in patients with metastatic breast cancer. J Clin Oncol. 1999; 17:2341–2354.
Article9. Baron RL, Oliver JH 3rd, Dodd GD 3rd, Nalesnik M, Holbert BL, Carr B. Hepatocellular carcinoma: evaluation with biphasic, contrast-enhanced, helical CT. Radiology. 1996; 199:505–511.
Article10. Semelka R, Ascher S, Reinhold C. MRI of the abdomen and pelvis: a text-atlas. New York: Wiley-Liss;1997.11. Koyama T, Fletcher JG, Johnson CD, Kuo MS, Notohara K, Burgart LJ. Primary hepatic angiosarcoma: findings at CT and MR imaging. Radiology. 2002; 222:667–673.
Article12. Rademaker J, Widjaja A, Galanski M. Hepatic hemangiosarcoma: imaging findings and differential diagnosis. Eur Radiol. 2000; 10:129–133.
Article13. Peterson MS, Baron RL, Rankin SC. Hepatic angiosarcoma: findings on multiphasic contrast-enhanced helical CT do not mimic hepatic hemangioma. AJR Am J Roentgenol. 2000; 175:165–170.14. White PG, Adams H, Smith PM. The computed tomographic appearances of angiosarcoma of the liver. Clin Radiol. 1993; 48:321–325.
Article15. Dunn GD, Hayes P, Breen KJ, Schenker S. The liver in congestive heart failure: a review. Am J Med Sci. 1973; 265:174–189.16. Van Beers B, Pringot J, Trigaux JP, Dautrebande J, Mathurin P. Hepatic heterogeneity on CT in Budd-Chiari syndrome: correlation with regional disturbances in portal flow. Gastrointest Radiol. 1988; 13:61–66.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Three Cases of Fulminant Hepatic Failure due to Congestive Heart Failure
- How to tackle congestion in acute heart failure
- Prenatal sonographic diagnosis of fetal hepatic hemangioma
- Biliary nonanastomosis stricture related with hepatic congestion in the right liver graft
- Acute Hepatic Failure after Spinal Surgery in Patient with Liver Cirrhosis: A case report
