Ann Lab Med.
2013 Nov;33(6):401-405. 10.3343/alm.2013.33.6.401.
Random Urinary Calcium/Creatinine Ratio for Screening Hypercalciuria in Children with Hematuria
- Affiliations
-
- 1Department of Pediatrics, Chonnam National University Medical School and Hospital, Gwangju, Korea. nuts99@naver.com
- KMID: 1711311
- DOI: http://doi.org/10.3343/alm.2013.33.6.401
Abstract
- BACKGROUND
Hypercalciuria is one of the most common causes of unexplained isolated hematuria. The diagnostic methods for hypercalciuria have not yet been standardized. The aim of this study was to assess whether random urinary calcium/creatinine ratio could be used as a screening tool for hypercalciuria in children with hematuria.
METHODS
This prospective study included 264 children with primary hematuria for whom both random and 24 hr urinary evaluations were performed. Pearson correlation and ROC curve were used to assess the correlations. A multiple linear regression model was used to analyze effects of age, weight, height, body mass index, and body surface area on random urinary calcium/creatinine ratio.
RESULTS
There was a moderately strong correlation between random urinary calcium/creatinine ratio and 24 hr urinary calcium excretion (r=0.584, P<0.001). The most appropriate cutoff value of random urinary calcium/creatinine ratio for the estimation of hypercalciuria was 0.075 mg/mg (sensitivity, 77.8%; specificity, 64.3%; area under the curve, 0.778). Body mass index and 24 hr urinary calcium excretion significantly affected random urinary calcium/creatinine ratio with a low coefficient of determination (r2=0.380, P<0.001).
CONCLUSIONS
Random urinary calcium/creatinine ratio is not suitable for screening hypercalciuria in children with hematuria. Twenty-four hour urinary analysis should be performed to diagnose hypercalciuria in children with hematuria.
Keyword
MeSH Terms
Figure
-
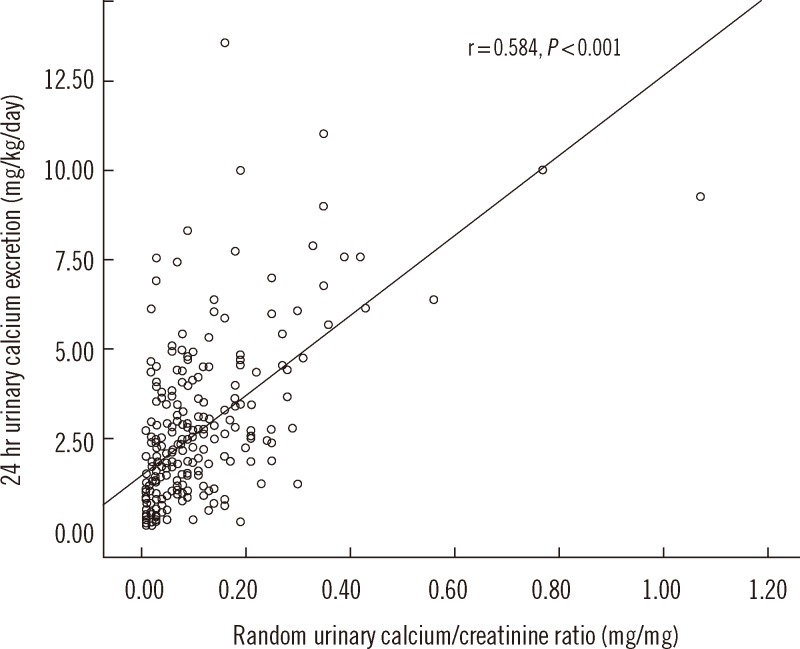
Fig. 1 Pearson correlation between random urinary calcium/creatinine ratio and 24 hr urinary calcium excretion. The Pearson coefficient (r) was 0.584 (P<0.001).
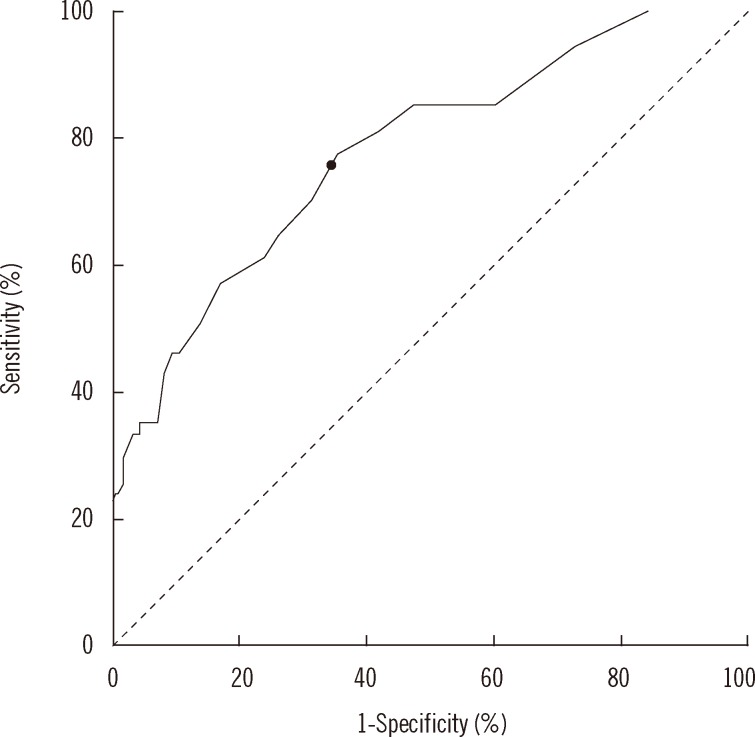
Fig. 2 Receiver operating characteristics curve analysis of random urinary calcium/creatinine ratio. The cut-off value (marked with a black dot on the curve) of random urinary calcium/creatinine ratio for detecting hypercalciuria was defined as 0.075 mg/mg (sensitivity, 77.8%; specificity, 64.3%; area under the curve, 0.778; P<0.001).
Reference
-
1. Feld LG, Meyers KE, Kaplan BS, Stapleton FB. Limited evaluation of microscopic hematuria in pediatrics. Pediatrics. 1998; 102:E42. PMID: 9755279.
Article2. Vachvanichsanong P, Malagon M, Moore ES. Recurrent abdominal and flank pain in children with idiopathic hypercalciuria. Acta Paediatr. 2001; 90:643–648. PMID: 11440097.
Article3. Zerwekh JE. Bone disease and hypercalciuria in children. Pediatr Nephrol. 2010; 25:395–401. PMID: 19885683.
Article4. Pace G, Aceto G, Cormio L, Traficante A, Tempesta A, Lospalluti ML, et al. Nocturnal enuresis can be caused by absorptive hypercalciuria. Scand J Urol Nephrol. 1999; 33:111–114. PMID: 10360451.5. Kaneko K, Tsuchiya K, Kawamura R, Ohtomo Y, Shimizu T, Yamashiro Y, et al. Low prevalence of hypercalciuria in Japanese children. Nephron. 2002; 91:439–443. PMID: 12119474.
Article6. Kaneko K, Chiba M, Hashizume M, Kunii O, Sasaki S, Shimoda T, et al. Extremely high prevalence of hypercalciuria in children living in the Aral Sea region. Acta Paediatr. 2002; 91:1116–1120. PMID: 12434899.
Article7. Ryu KH, Lee SJ, Lee K, Jung JS. Idiopathic hypercalciuria in children. J Korean Pediatr Soc. 1989; 32:809–815.8. Ahn YH, Kim KH, Ko CW, Koo JH. Idiopathic hypercalciuria in children. Korean J Nephrol. 1989; 8:79–84.9. Ghazali S, Barratt TM. Urinary excretion of calcium and magnesium in children. Arch Dis Child. 1974; 49:97–101. PMID: 4406087.
Article10. Arrabal-Polo MA, Arias-Santiago S, Girón-Prieto MS, Abad-Menor F, López-Carmona Pintado F, Zuluaga-Gomez A, et al. Hypercalciuria, hyperoxaluria, and hypocitraturia screening from random urine samples in patients with calcium lithiasis. Urol Res. 2012; 40:511–515. PMID: 22484727.
Article11. Koyun M, Güven AG, Filiz S, Akman S, Akbas H, Baysal YE, et al. Screening for hypercalciuria in schoolchildren: what should be the criteria for diagnosis? Pediatr Nephrol. 2007; 22:1297–1301. PMID: 17549524.
Article12. Hong YH, Dublin N, Razack AH, Mohd MA, Husain R. Twenty-four hour and spot urine metabolic evaluations: correlations versus agreements. Urology. 2010; 75:1294–1298. PMID: 19914693.
Article13. Matos V, van Melle G, Boulat O, Markert M, Bachmann C, Guignard JP. Urinary phosphate/creatinine, calcium/creatinine, and magnesium/creatinine ratios in a healthy pediatric population. J Pediatr. 1997; 131:252–257. PMID: 9290612.
Article14. Safarinejad MR. Urinary mineral excretion in healthy Iranian children. Pediatr Nephrol. 2003; 18:140–144. PMID: 12579403.
Article15. Sönmez F, Akcanal B, Altincik A, Yenisey C. Urinary calcium excretion in healthy Turkish children. Int Urol Nephrol. 2007; 39:917–922. PMID: 17043921.
Article16. Ahn HS, Suh BK, Seo JK, Oh SH, Lee SI, Lee C, editors. Textbook of Pediatrics. 10th ed. Seoul: Miraen Publishing Co.;2012. p. 916–917.17. Mir S, Serdaroqlu E. Quantification of hypercalciuria with the urine calcium osmolality ratio in children. Pediatr Nephrol. 2005; 20:1562–1565. PMID: 16133062.
Article18. Mosteller RD. Simplified calculation of body-surface area. N Engl J Med. 1987; 317:1098. PMID: 3657876.
Article19. Reusz GS, Dobos M, Byrd D, Sallay P, Miltenyi M, Tulassay T. Urinary calcium and oxalate excretion in children. Pediatr Nephrol. 1995; 9:39–44. PMID: 7742220.
Article20. Alconcher LF, Castro C, Quintana D, Abt N, Moran L, Gonzalez L, et al. Urinary calcium excretion in healthy school children. Pediatr Nephrol. 1997; 11:186–188. PMID: 9090660.
Article21. Esbjörner E, Jones IL. Urinary calcium excretion in Swedish children. Acta Paediatr. 1995; 84:156–159. PMID: 7756801.22. Sargent JD, Stukel TA, Kresel J, Klein RZ. Normal values for random urinary calcium to creatinine ratios in infancy. J Pediatr. 1993; 123:393–397. PMID: 8355114.
Article23. Remer T, Neubert A, Maser-Gluth C. Anthropometry-based reference values for 24-hr urinary creatinine excretion during growth and their use in endocrine and nutritional research. Am J Clin Nutr. 2002; 75:561–569. PMID: 11864864.24. Mori Y, Hiraoka M, Suganuma N, Tsukahara H, Yoshida H, Mayumi M. Urinary creatinine excretion and protein/creatinine ratios vary by body size and gender in children. Pediatr Nephrol. 2006; 21:683–687. PMID: 16550362.
Article25. Manz F, Kehrt R, Lausen B, Merkel A. Urinary calcium excretion in healthy children and adolescents. Pediatr Nephrol. 1999; 13:894–899. PMID: 10603144.
Article26. Seifert-McLean CM, Cromer BA, Mosher G, Mahan JD. Urinary calcium excretion in healthy adolescents. J Adolesc Health Care. 1989; 10:300–304. PMID: 2732110.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Two Cases of Idiopathic Hypercalciuria in Children with Hematuria
- Determination of Urinary cAMP in the Patients with Urinary Stones
- Clinical Evaluation of Hypercalciuria and Hematuria in NIDDM
- Comparison of Blood and Urine Renal Indices Between Hypercalciuric and Non-hypercalciuric Hematuria Patients
- Nocturnal Hypercalciuria for Enuresis Subtypes: Prospective Controlled Study
