Differentiating between Adenomyomatosis and Gallbladder Cancer: Revisiting a Comparative Study of High-Resolution Ultrasound, Multidetector CT, and MR Imaging
- Affiliations
-
- 1Department of Radiology and the Institute of Radiation Medicine, Seoul National University Hospital, Seoul 110-744, Korea. leejy4u@snu.ac.kr
- KMID: 1705577
- DOI: http://doi.org/10.3348/kjr.2014.15.2.226
Abstract
OBJECTIVE
To compare the diagnostic performance of high-resolution ultrasound (HRUS) with contrast-enhanced CT and contrast-enhanced magnetic resonance imaging (MRI) with MR cholangiopancreatography (MRCP) to differentiate between adenomyomatosis (ADM) and gallbladder cancer (GBCA).
MATERIALS AND METHODS
Forty patients with surgically proven ADM (n = 13) or GBCA at stage T2 or lower (n = 27) who previously underwent preoperative HRUS, contrast-enhanced CT, and contrast-enhanced MRI with MRCP were retrospectively included in this study. According to the well-known diagnostic criteria, two reviewers independently analyzed the images from each modality separately with a five-point confidence scale. The interobserver agreement was calculated using weighted kappa statistics. A receiver operating characteristic curve analysis was performed and the sensitivity, specificity, and accuracy were calculated for each modality when scores of 1 or 2 indicated ADM.
RESULTS
The interobserver agreement between the two reviewers was good to excellent. The mean Az values for HRUS, multidetector CT (MDCT), and MRI were 0.959, 0.898, and 0.935, respectively, without any statistically significant differences between any of the modalities (p > 0.05). The mean sensitivity of MRI with MRCP (80.8%) was significantly higher than that of MDCT (50.0%) (p = 0.0215). However, the mean sensitivity of MRI with MRCP (80.8%) was not significantly different from that of HRUS (73.1%) (p > 0.05). The mean specificities and accuracies among the three modalities were not significantly different (p > 0.05).
CONCLUSION
High-resolution ultrasound and MRI with MRCP have comparable sensitivity and accuracy and MDCT has the lowest sensitivity and accuracy for the differentiation of ADM and GBCA.
MeSH Terms
-
Adenomyoma/*diagnosis
Adult
Aged
Aged, 80 and over
Cholangiopancreatography, Magnetic Resonance/methods
Contrast Media/diagnostic use
Diagnosis, Differential
Diagnostic Imaging/*methods
Female
Gallbladder Neoplasms/*diagnosis
Humans
Magnetic Resonance Imaging/methods
Male
Middle Aged
Observer Variation
ROC Curve
Retrospective Studies
Sensitivity and Specificity
Tomography, X-Ray Computed/methods
Ultrasonography/methods
Contrast Media
Figure
-

Fig. 1 Fundal adenomyoma of gallbladder in 62-year-old male. A. MR image with thick-slab, T2-weighted fast spin-echo sequence shows typical "pearl necklace sign" at fundus of gallbladder (arrows). B. CT image during portal venous phase demonstrates fundal abnormality with enhancing epithelium and multiple intramural cystic lesions (Rosary sign) (arrows). C. High resolution ultrasound image showing multiple intramural cysts (arrows) within thickened wall at fundus.
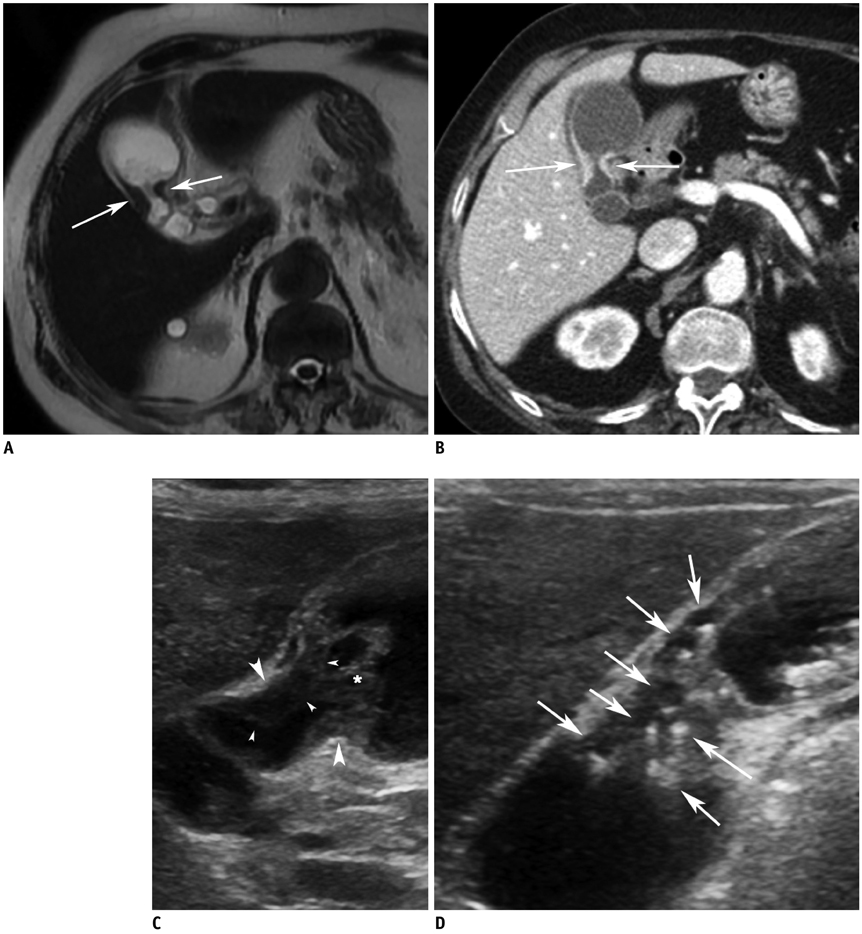
Fig. 2 Gallbladder body cancer (pT2) in 81-year-old female. A. MR image with T2-weighted single-shot fast spin-echo sequence shows segmental thickening (arrows) without evidence of intramural cysts at body of gallbladder. B. CT image during portal venous phase shows segmental wall thickening with strong contrast enhancement at body (arrows). C. High-resolution ultrasound image showing segmental wall thickening (arrowheads) without evidence of intramural cysts or intramural echogenic material deposition at body. Asterisks (*) indicate sludge. D. High-resolution ultrasound image in patient with segmental adenomyomatosis shows multiple cysts and echogenic materials (arrows) within thickened walls. This image clearly shows difference between adenomyomatosis and cancer on ultrasound image.
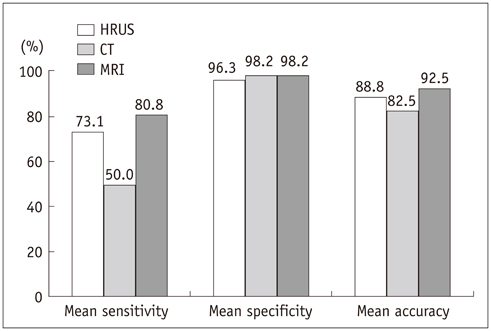
Fig. 3 Bar graph displaying mean sensitivities, specificities, and accuracies of high-resolution ultrasound (HRUS), CT, and MRI for diagnosis of adenomyomatosis of gallbladder.
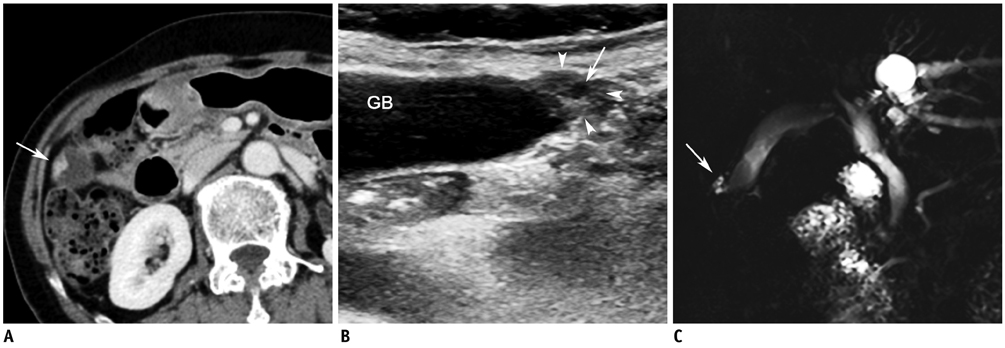
Fig. 4 Fundal adenomyoma in 72-year-old female. A. CT image during portal venous phase showing focal wall thickening with heterogeneous contrast enhancement (arrow) at fundus of GB. B. High-resolution ultrasound image showing focal thickening at fundus (arrowheads) containing cystic lesion (arrow), indicating presence of dilated intramural Rokitansky-Aschoff sinuses. C. MR image with thick-slab, T2-weighted fast spin-echo sequence demonstrating focal high signal intensity lesion (arrow), indicating presence of dilated intramural Rokitansky-Aschoff sinuses at fundus. GB = gallbladder

Fig. 5 Adenomyomatosis in GB fundus in 61-year-old female. A. CT image during portal venous phase showing marked wall thickening with strong contrast enhancement (arrow) at fundus of GB. There is no evidence of intramural cysts. B. T1-weighted MR image during portal venous phase also shows diffuse thickening at fundus with strong contrast enhancement (arrow). There is no evidence of intramural cysts on T2-weighted images (not shown). C. High-resolution ultrasound image shows diffuse wall thickening at fundus with multiple intramural deposition of echogenic materials (arrows) which represent intramural cholesterol crystal deposition. This finding favors diagnosis of adenomyomatosis more than GB cancer. GB = gallbladder
Reference
-
1. Jutras JA. Hyperplastic cholecystoses; Hickey lecture, 1960. Am J Roentgenol Radium Ther Nucl Med. 1960; 83:795–827.2. Colquhoun J. Adenomyomatosis of the gall-bladder (intramural diverticulosis). Br J Radiol. 1961; 34:101–112.3. Fotopoulos JP, Crampton AR. Adenomyomatosis of the gallbladder. Med Clin North Am. 1964; 48:9–36.4. Williams I, Slavin G, Cox A, Simpson P, de Lacey G. Diverticular disease (adenomyomatosis) of the gallbladder: a radiological-pathological survey. Br J Radiol. 1986; 59:29–34.5. Gerard PS, Berman D, Zafaranloo S. CT and ultrasound of gallbladder adenomyomatosis mimicking carcinoma. J Comput Assist Tomogr. 1990; 14:490–491.6. Ching BH, Yeh BM, Westphalen AC, Joe BN, Qayyum A, Coakley FV. CT differentiation of adenomyomatosis and gallbladder cancer. AJR Am J Roentgenol. 2007; 189:62–66.7. Yoshimitsu K, Honda H, Aibe H, Shinozaki K, Kuroiwa T, Irie H, et al. Radiologic diagnosis of adenomyomatosis of the gallbladder: comparative study among MRI, helical CT, and transabdominal US. J Comput Assist Tomogr. 2001; 25:843–850.8. Oktar SO, Yücel C, Ozdemir H, Ulutürk A, Işik S. Comparison of conventional sonography, real-time compound sonography, tissue harmonic sonography, and tissue harmonic compound sonography of abdominal and pelvic lesions. AJR Am J Roentgenol. 2003; 181:1341–1347.9. Dahl JJ, Soo MS, Trahey GE. Clinical evaluation of combined spatial compounding and adaptive imaging in breast tissue. Ultrason Imaging. 2004; 26:203–216.10. Yen CL, Jeng CM, Yang SS. The benefits of comparing conventional sonography, real-time spatial compound sonography, tissue harmonic sonography, and tissue harmonic compound sonography of hepatic lesions. Clin Imaging. 2008; 32:11–15.11. Jang JY, Kim SW, Lee SE, Hwang DW, Kim EJ, Lee JY, et al. Differential diagnostic and staging accuracies of high resolution ultrasonography, endoscopic ultrasonography, and multidetector computed tomography for gallbladder polypoid lesions and gallbladder cancer. Ann Surg. 2009; 250:943–949.12. Yoon SH, Lee JM, So YH, Hong SH, Kim SJ, Han JK, et al. Multiphasic MDCT enhancement pattern of hepatocellular carcinoma smaller than 3 cm in diameter: tumor size and cellular differentiation. AJR Am J Roentgenol. 2009; 193:W482–W489.13. Rice J, Sauerbrei EE, Semogas P, Cooperberg PL, Burhenne HJ. Sonographic appearance of adenomyomatosis of the gallbladder. J Clin Ultrasound. 1981; 9:336–337.14. Raghavendra BN, Subramanyam BR, Balthazar EJ, Horii SC, Megibow AJ, Hilton S. Sonography of adenomyomatosis of the gallbladder: radiologic-pathologic correlation. Radiology. 1983; 146:747–752.15. Brambs HJ, Wrazidlo W, Schilling H. [The sonographic image of gallbladder adenomyomatosis]. Rofo. 1990; 153:633–636.16. Hwang JI, Chou YH, Tsay SH, Chiang JH, Chang CY, Boland GW, et al. Radiologic and pathologic correlation of adenomyomatosis of the gallbladder. Abdom Imaging. 1998; 23:73–77.17. Boscak AR, Al-Hawary M, Ramsburgh SR. Best cases from the AFIP: adenomyomatosis of the gallbladder. Radiographics. 2006; 26:941–946.18. Clouston JE, Thorpe RJ. Case report--CT findings in adenomyomatosis of the gallbladder. Australas Radiol. 1991; 35:86–87.19. Chao C, Hsiao HC, Wu CS, Wang KC. Computed tomographic finding in adenomyomatosis of the gallbladder. J Formos Med Assoc. 1992; 91:467–469.20. Stunell H, Buckley O, Geoghegan T, O'Brien J, Ward E, Torreggiani W. Imaging of adenomyomatosis of the gall bladder. J Med Imaging Radiat Oncol. 2008; 52:109–117.21. Miyazaki T, Yamashita Y, Tsuchigame T, Yamamoto H, Urata J, Takahashi M. MR cholangiopancreatography using HASTE (half-Fourier acquisition single-shot turbo spin-echo) sequences. AJR Am J Roentgenol. 1996; 166:1297–1303.22. Yoshimitsu K, Honda H, Jimi M, Kuroiwa T, Hanada K, Irie H, et al. MR diagnosis of adenomyomatosis of the gallbladder and differentiation from gallbladder carcinoma: importance of showing Rokitansky-Aschoff sinuses. AJR Am J Roentgenol. 1999; 172:1535–1540.23. Haradome H, Ichikawa T, Sou H, Yoshikawa T, Nakamura A, Araki T, et al. The pearl necklace sign: an imaging sign of adenomyomatosis of the gallbladder at MR cholangiopancreatography. Radiology. 2003; 227:80–88. questionnaire, 549-555.24. Levy AD, Murakata LA, Rohrmann CA Jr. Gallbladder carcinoma: radiologic-pathologic correlation. Radiographics. 2001; 21:295–314.25. Metz CE. Some practical issues of experimental design and data analysis in radiological ROC studies. Invest Radiol. 1989; 24:234–245.26. Gore RM, Yaghmai V, Newmark GM, Berlin JW, Miller FH. Imaging benign and malignant disease of the gallbladder. Radiol Clin North Am. 2002; 40:1307–1323. vi27. Lee JY, Choi BI, Han JK, Lee JM, Kim SH, Choi JY, et al. High resolution ultrasonographic evaluation of the gallbladder: value of advanced imaging techniques. J Korean Soc Ultrasound Med. 2005; 24:169–175.28. Liasis N, Klonaris C, Katsargyris A, Georgopoulos S, Labropoulos N, Tsigris C, et al. The use of Speckle Reduction Imaging (SRI) Ultrasound in the characterization of carotid artery plaques. Eur J Radiol. 2008; 65:427–433.29. Oria HE. Pitfalls in the diagnosis of gallbladder disease in clinically severe obesity. Obes Surg. 1998; 8:444–451.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Adenocarcinoma Arising in Segmental Adenomyomatosis of the Gallbladder: A Case Report
- Report of a Case of Adenomyomatosis of Gallbladder
- Ultrasound of the Gallbladder
- Focal Thickening at the Fundus of the Gallbladder: Computed Tomography Differentiation of Fundal Type Adenomyomatosis and Localized Chronic Cholecystitis
- Localized Adenomyomatosis of Gallbladder Mimicking Advanced Hepatic Flexure Colon Cancer: A Case Report
