Localized Adenomyomatosis of Gallbladder Mimicking Advanced Hepatic Flexure Colon Cancer: A Case Report
- Affiliations
-
- 1Department of Radiology, Ajou University School of Medicine, Ajou University Hospital, Suwon, Korea. kbh@ajou.ac.kr
- 2Department of Pathology, Ajou University School of Medicine, Ajou University Hospital, Suwon, Korea.
- 3Department of Gastroenterology, Ajou University School of Medicine, Ajou University Hospital, Suwon, Korea.
- KMID: 2422908
- DOI: http://doi.org/10.3348/jksr.2018.79.5.290
Abstract
- Localized forms of gallbladder adenomyomatosis are rarely polypoid and may mimic gallbladder cancer. Herein, we present a unique case of polypoid gallbladder adenomyomatosis penetrating the colon and preoperatively misdiagnosed as advanced hepatic flexure colon cancer.
Figure
-
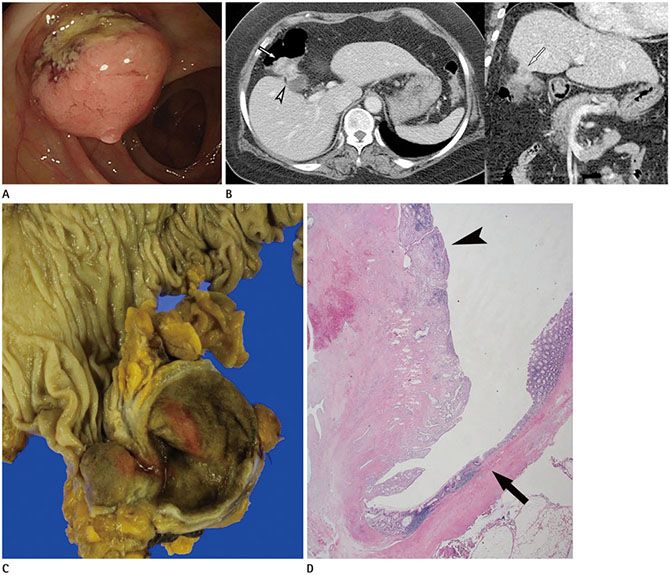
Fig. 1 Localized adenomyomatosis of gallbladder in 62-year-old female patient initially misdiagnosed as an advanced hepatic flexure colon cancer. A. The colonoscopy shows a 3 cm polypoid mass with ulceration, mucosal denudation in the stalk, and the mucosa of the mass is different from the colonic mucosa. B. Axial image of contrast enhanced CT scan depicts a heterogeneous enhancing intraluminal polypoid mass in the hepatic flexure of the colon (arrow), with extension to the adjacent gallbladder fundus (arrowhead). On coronal image, this mass is closely abutting the adjacent liver parenchyma, causing tethered appearance of the liver surface (arrow). Colon cancer with gallbladder and liver invasion was highly suspected. C. Gross specimen shows brownish polypoid mass arising from the gallbladder, same color as gallbladder mucosa. D. Photomicrograph reveals the mass composed of gallbladder mucosa (arrowhead), connected to the atrophied colonic mucosa (arrow). Rokitansky-Aschoff sinuses are located in the hypertrophied muscular layer, suggesting adenomyomatous hyperplasia (hematoxylin and eosin stain, × 40).
Reference
-
1. Miyazaki K, Tsutsumi N, Sasatomi E, Kitahara K, Mori M, Tokunaga O, et al. Benign gallbladder lesions mimicking cancer infiltrating the liver. J Hepatobiliary Pancreat Surg. 1994; 1:273–279.
Article2. Gerard PS, Berman D, Zafaranloo S. CT and ultrasound of gallbladder adenomyomatosis mimicking carcinoma. J Comput Assist Tomogr. 1990; 14:490–491.3. Mellnick VM, Menias CO, Sandrasegaran K, Hara AK, Kielar AZ, Brunt EM, et al. Polypoid lesions of the gallbladder: disease spectrum with pathologic correlation. Radiographics. 2015; 35:387–399.4. Levy AD, Murakata LA, Rohrmann CA Jr. Gallbladder carcinoma: radiologic-pathologic correlation. Radiographics. 2001; 21:295–314. questionnaire, 549-555.
Article5. Landmann RG, Weiser MR. Surgical management of locally advanced and locally recurrent colon cancer. Clin Colon Rectal Surg. 2005; 18:182–189.
Article6. Glenn F, Reed C, Grafe WR. Biliary enteric fistula. Surg Gynecol Obstet. 1981; 153:527–531.7. Haff RC, Wise L, Ballinger WF. Biliary-enteric fistulas. Surg Gynecol Obstet. 1971; 133:84–88.8. Costi R, Randone B, Violi V, Scatton O, Sarli L, Soubrane O, et al. Cholecystocolonic fistula: facts and myths. A review of the 231 published cases. J Hepatobiliary Pancreat Surg. 2009; 16:8–18.
Article9. Ha GW, Lee MR, Kim JH. Cholecystocolic fistula caused by gallbladder carcinoma: preoperatively misdiagnosed as hepatic colon carcinoma. World J Gastroenterol. 2015; 21:4765–4769.
Article10. Mann CD, Johnson NA, Metcalfe MS, Neal CP, Harrison RF, Berry DP, et al. Cholecystobronchial fistula secondary to adenomyomatosis of the gallbladder. Ann R Coll Surg Engl. 2007; 89:W14–W16.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Adenocarcinoma Arising in Segmental Adenomyomatosis of the Gallbladder: A Case Report
- Synchronous Cancers of Hepatic Angiosarcoma and Gallbladder Adenocarcinoma, Mimicking Gallbladder Cancer with Hepatic Invasion: a Case Report
- Focal Thickening at the Fundus of the Gallbladder: Computed Tomography Differentiation of Fundal Type Adenomyomatosis and Localized Chronic Cholecystitis
- Report of a Case of Adenomyomatosis of Gallbladder
- Hepatic Arterial Infusion Chemotherapy Using the Port System in Advanced Gallbladder Cancer
