Tuberc Respir Dis.
2007 Mar;62(3):217-222. 10.4046/trd.2007.62.3.217.
Two Cases of Fatal Hypoxemia after Talc Pleurodesis for Recurrent Malignant Pleural Effusion
- Affiliations
-
- 1Department of Internal Medicine, The Catholic University or Korea, Suwon, Korea. kimhoonkyo@yahoo.co.kr
- 2Department of Radiology, The Catholic University or Korea, Suwon, Korea.
- 3Department of Thoracic Surgery College of Medicine, The Catholic University or Korea, Suwon, Korea.
- KMID: 1518467
- DOI: http://doi.org/10.4046/trd.2007.62.3.217
Abstract
- Talc pleurodesis is a safe and effective treatment for a recurrent malignant pleural effusion. However, acute hypoxemia, pulmonary edema or acute respiratory failure can develop in a small number of patients. We report 2 patients who developed fatal hypoxemia after talc pleurodesis which was necessary the control recurrent pleural effusion. The first case was an 18-year old male diagnosed with Ewing's sarcoma with bilateral lung metastases and pleural effusion. The performance status was ECOG (Eastern Cooperative Foncology Group) grade 3. Fever along with hypoxemia and leukocytosis developed 10 hours after the second talc pleurodesis on the right side for an uncontrolled pleural effusion, The patient died from respiratory failure after 13 days. The second case was a 66-year old female diagnosed with non-small cell lung cancer with a bone metastasis. Two weeks after systemic chemotherapy, she complained of dyspnea, and a pleural effusion was observed on the right side. Her performance status was ECOG grade 3. Talc pleurodesis was performed for recurrent pleural effusion, but hypoxemia developed 6 days after pleurodesis and she died from respiratory failure 10 days after pleurodesis. In conclusion, talc pleurodesis should be performed very carefully in patients with a poor performance status, in cases with repeated pleurodesis, bilateral pleural effusion, recent chemotherapy, radiotherapy and when there are parenchymal metastatic lesions present.
Keyword
MeSH Terms
Figure
-

Figure 1 Chest PA shows moderate amount of right pleural effusion, left pleural thickening and left lung infiltration before right talc pleurodesis.
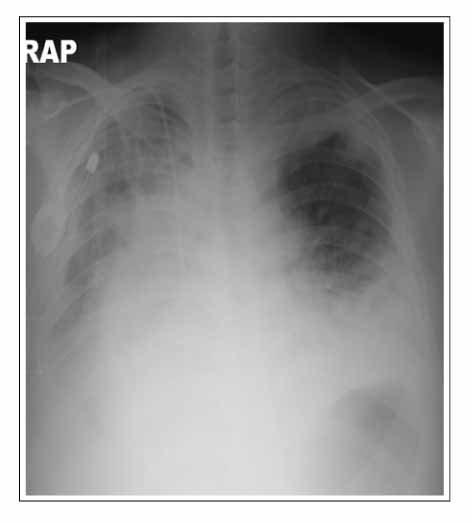
Figure 2 Chest PA shows increased amount of right pleural effusion, interstitial infiltrations and after talc pleurodesis.

Figure 3 Chest PA & right decubitus view show loculated right pleural effusion before pleurodesis.

Figure 4 Chest CT shows a 5.4×4.5 cm mass in the right lower lobe and surrounding atelectasis in right middle lobe. Large amount of right pleural effusion is noted before pleurodesis.

Figure 5 Chest PA shows multifocal patch consolidation and haziness in both lungs after talc pleurodesis.
Reference
-
1. Bondoc AY, Bach PB, Sklarin NT, Vander Els NJ. Arterial desaturation syndrome following pleurodesis with talc slurry: incidence, clinical features, and outcome. Cancer Invest. 2003. 21:848–854.2. Kim KU, Cha KY, Han SH, Yun YI, Park SW, Kim DJ, et al. A case of acute respiratory distress syndrome (ARDS) after talc pleurodesis. Tuberc Respir Dis. 2001. 51:265–269.3. Brega-Massone PP, Lequaglie C, Magnani B, Ferro F, Cataldo I. Chemical pleurodesis to improve patients' quality of life in the management of malignant pleural effusions: the 15 year experience of the National Cancer Institute of Milan. Surg Laparosc Endosc Percutan Tech. 2004. 14:73–79.4. Antunes G, Neville E. Management of malignant pleural effusions. Thorax. 2000. 55:981–983.5. Antony VB, Nasreen N, Mohammed KA, Sriram PS, Frank W, Schoenfeld N, et al. Talc pleurodesis: basic fibroblast growth factor mediates pleural fibrosis. Chest. 2004. 126:1522–1528.6. Marchi E, Teixeira LR, Vargas FS. Management of malignancy-associated pleural effusion: current and future treatment strategies. Am J Respir Med. 2003. 2:261–273.7. Kennedy L, Rusch VW, Strange C, Ginsberg RJ, Sahn SA. Pleurodesis using talc slurry. Chest. 1994. 106:342–346.8. Lee YC, Light RW. Management of malignant pleural effusions. Respirology. 2004. 9:148–156.9. Rehse DH, Aye RW, Florence MG. Respiratory failure following talc pleurodesis. Am J Surg. 1999. 177:437–440.10. Yim AP, Chan AT, Lee TW, Wan IY, Ho JK. Thoracoscopic talc insufflation versus talc slurry for symptomatic malignant pleural effusion. Ann Thorac Surg. 1996. 62:1655–1658.11. Viallat JR, Rey F, Astoul P, Boutin C. Thoracoscopic talc poudrage pleurodesis for malignant effusions: a review of 360 cases. Chest. 1996. 110:1387–1393.12. Neragi-Miandoab S. Malignant pleural effusion, current and evolving approaches for its diagnosis and management. Lung Cancer. 2006. 54:1–9.13. Bernard A, de Dompsure RB, Hagry O, Favre JP. Early and late mortality after pleurodesis for malignant pleural effusion. Ann Thorac Surg. 2002. 74:213–217.14. Kuzniar TJ, Blum MG, Kasibowska-Kuzniar K, Mutlu GM. Predictors of acute lung injury and severe hypoxemia in patients undergoing operative talc pleurodesis. Ann Thorac Surg. 2006. 82:1976–1981.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Acute Respirtory Distress Syndrome(ARDS) after Talc Pleurodesis
- Spontaneous Regression of Metastatic Renal Cell Carcinoma after Talc Pleurodesis
- Viscum Album Therapy in Malignant Pleural Effusion
- Which is the More Effective Option for Pleurodesis to Prevent the Recurrence of Malignant Pleural Effusion? Large-Particle Talc or Mistletoe Extract (ABNOVA Viscum Injection)
- Pleural Changes after Talc Pleurodesis in Patients with Underlying Malignancy: Comparison with Recurrent Malignant Pleural Lesions on CT and Fluorodeoxyglucose-Positron Emission Tomography/CT
