Pleural Changes after Talc Pleurodesis in Patients with Underlying Malignancy: Comparison with Recurrent Malignant Pleural Lesions on CT and Fluorodeoxyglucose-Positron Emission Tomography/CT
- Affiliations
-
- 1Department of Radiology, Kosin University Gospel Hospital, Busan, Korea. soinvain@naver.com
- KMID: 1897258
- DOI: http://doi.org/10.3348/jksr.2014.70.1.35
Abstract
- PURPOSE
To compare computed tomography (CT) and fluorodeoxyglucose-positron emission tomography/CT (FDG-PET/CT) findings of benign pleural changes with those of recurrent malignant pleural lesions in patients with a history of underlying malignancy after talc pleurodesis.
MATERIALS AND METHODS
Of 194 patients who underwent talc pleurodesis, we retrospectively reviewed 16 patients for whom both follow-up CT and FDG-PET/CT were performed. The morphologic CT findings and maximum standard uptake values (SUVmax) were evaluated and compared between benign pleural changes and recurrent malignant pleural lesions.
RESULTS
Twenty-two lesions were found in 16 patients; six patients had no evidence of active pleural disease (group 1) and 10 patients had recurrent malignant pleural lesions on radiological or clinical follow-up (group 2). Characteristic high-density pleural deposits [mean, 131 Hounsfield unit (HU); range, 28-251 HU] were seen along the pleural thickenings (mean, 13.4 mm; range, 4.9-62.3 mm) in 15 patients. The shape and thickness on CT and the SUVmax on FDG-PET/CT showed no significant differences between the two groups. On CT, the pre-contrast attenuation was higher in group 1 than group 2 (165 HU vs. 101 HU, respectively, p = 0.030), and the degree of enhancement was higher in group 2 than that in group 1 (29 HU vs. 48 HU, respectively, p = 0.048). Pleural effusions (n = 5) and other pleural thickening without high-density foci (n = 4) were observed only in group 2; however, no statistical significance was observed between the two groups.
CONCLUSION
Malignant pleural lesions can be characterized by lower pre-contrast attenuation and higher contrast enhancement, whereas benign pleural changes after talc pleurodesis are characterized by higher pre-contrast attenuation and lower contrast enhancement on CT.
MeSH Terms
Figure
-
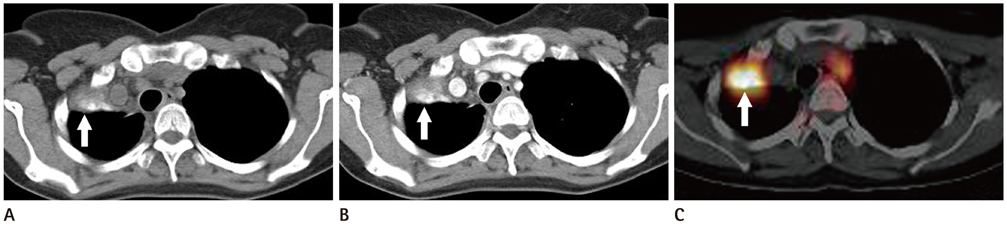
Fig. 1 A 49-year-old woman who underwent a right lower lobectomy due to lung adenocarcinoma (group 1). A. Pre-contrast CT scan taken 14 months after talc pleurodesis shows nodular pleural thickening with a focal area of high attenuation in the right upper thorax (arrow). B. Contrast-enhanced CT scan shows contrast enhancement (arrow). C. FDG-PET/CT scan shows intense FDG uptake (arrow). Note.-FDG-PET/CT = fluorodeoxyglucose-positron emission tomography/CT
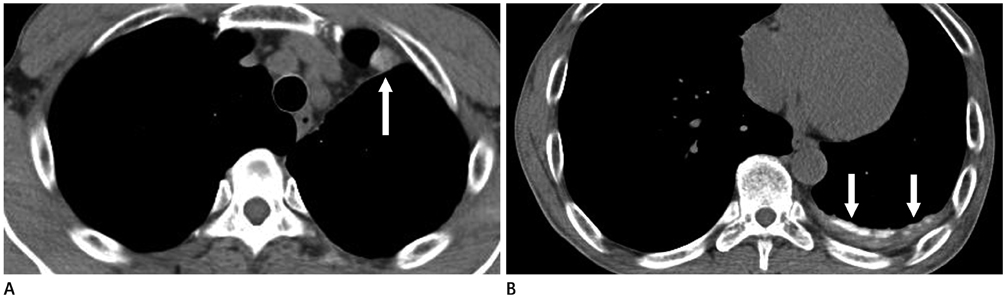
Fig. 2 A 53-year-old man who underwent a left lower lobectomy due to lung adenocarcinoma (group 1). A. Pre-contrast CT scan taken 20 months after talc pleurodesis shows a focal area of high attenuation with nodular pleural thickening in the left upper anterior thorax (arrow). B. Diffuse pleural thickening with a linear high attenuation area was seen in the left lower posterior thorax (arrows).

Fig. 3 A 65-year-old man who underwent right upper wedge resection due to squamous cell lung cancer (group 2). A, B. Pre-contrast (A) and contrast-enhanced (B) CT scans taken 3 months after talc pleurodesis show a high-density pleural thickening with patchy distribution and contrast enhancement in the right upper hemithorax (arrow). C. Contrast-enhanced CT scans taken 10 months after talc pleurodesis show a recurrent mass with pleural involvement in the right upper hemithorax.

Fig. 4 A 77-year-old woman with malignant mesothelioma (group 2). A. Contrast-enhanced CT scan taken 3 months after talc pleurodesis shows an area of high density with pleural thickening in the left hemithorax. B. Eighteen months later, enhancing pleural thickening and nodules arose from the previously noted high-density pleural lesion (arrows).
Reference
-
1. Rodriguez-Panadero F, Montes-Worboys A. Mechanisms of pleurodesis. Respiration. 2012; 83:91–98.2. Narayanaswamy S, Kamath S, Williams M. CT appearances of talc pleurodesis. Clin Radiol. 2007; 62:233–237.3. Shaw P, Agarwal R, et al. Pleurodesis for malignant pleural effusions. Cochrane Database Syst Rev. 2004; CD002916.4. Tan C, Sedrakyan A, Browne J, Swift S, Treasure T. The evidence on the effectiveness of management for malignant pleural effusion: a systematic review. Eur J Cardiothorac Surg. 2006; 29:829–838.5. Murray JG, Patz EF Jr, Erasmus JJ, Gilkeson RC. CT appearance of the pleural space after talc pleurodesis. AJR Am J Roentgenol. 1997; 169:89–91.6. Williams T, Gostelow B, Woods D, Spyt T. Apical pleural mass developing following talc pleurodesis. Respir Med. 1998; 92:358–359.7. Avila NA, Dwyer AJ, Rabel A, DeCastro RM, Moss J. CT of pleural abnormalities in lymphangioleiomyomatosis and comparison of pleural findings after different types of pleurodesis. AJR Am J Roentgenol. 2006; 186:1007–1012.8. Murray JG, Erasmus JJ, Bahtiarian EA, Goodman PC. Talc pleurodesis simulating pleural metastases on 18F-fluorodeoxyglucose positron emission tomography. AJR Am J Roentgenol. 1997; 168:359–360.9. Weiss N, Solomon SB. Talc pleurodesis mimics pleural metastases: differentiation with positron emission tomography/computed tomography. Clin Nucl Med. 2003; 28:811–814.10. Kwek BH, Aquino SL, Fischman AJ. Fluorodeoxyglucose positron emission tomography and CT after talc pleurodesis. Chest. 2004; 125:2356–2360.11. Nguyen M, Varma V, Perez R, Schuster DM. CT with histopathologic correlation of FDG uptake in a patient with pulmonary granuloma and pleural plaque caused by remote talc pleurodesis. AJR Am J Roentgenol. 2004; 182:92–94.12. Ahmadzadehfar H, Palmedo H, Strunk H, Biersack HJ, Habibi E, Ezziddin S. False positive 18F-FDG-PET/CT in a patient after talc pleurodesis. Lung Cancer. 2007; 58:418–421.13. Al-Sarraf N, Doddakula K, Wedde T, Young V. Positron emission tomography staging of pleural deposits following Monaldi's procedure: an accurate reflection or a false staging? Interact Cardiovasc Thorac Surg. 2007; 6:260–261.14. Nguyen NC, Tran I, Hueser CN, Oliver D, Farghaly HR, Osman MM. F-18 FDG PET/CT characterization of talc pleurodesis-induced pleural changes over time: a retrospective study. Clin Nucl Med. 2009; 34:886–890.15. Peek H, van der Bruggen W, Limonard G. Pleural FDG Uptake More Than a Decade after Talc Pleurodesis. Case Rep Med. 2009; 2009:650864.16. Tenconi S, Luzzi L, Paladini P, Voltolini L, Gallazzi MS, Granato F, et al. Pleural granuloma mimicking malignancy 42 years after slurry talc injection for primary spontaneous pneumothorax. Eur Surg Res. 2010; 44:201–203.17. Bethune N. Pleural poudrage. A new technique for the deliberate production of pleural adhesions as a preliminary to lobectomy. J Thorac Surg. 1935; 4:251–261.18. Jones GR. Treatment of recurrent malignant pleural effusion by iodized talc pleurodesis. Thorax. 1969; 24:69–73.19. Ahmed Z, Shrager JB. Mediastinal talcoma masquerading as thymoma. Ann Thorac Surg. 2003; 75:568–569.20. De Weerdt S, Noppen M, Everaert H, Vincken W. Positron emission tomography scintigraphy after thoracoscopic talcage. Respiration. 2004; 71:284.21. Leung AN, Müller NL, Miller RR. CT in differential diagnosis of diffuse pleural disease. AJR Am J Roentgenol. 1990; 154:487–492.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Acute Respirtory Distress Syndrome(ARDS) after Talc Pleurodesis
- Spontaneous Regression of Metastatic Renal Cell Carcinoma after Talc Pleurodesis
- Two Cases of Fatal Hypoxemia after Talc Pleurodesis for Recurrent Malignant Pleural Effusion
- Malignant Pleural Mesothelioma Diagnosed by Endobronchial Ultrasound-Guided Transbronchial Needle Aspiration
- Viscum Album Therapy in Malignant Pleural Effusion
