A Case of Pulmonary Alveolar Proteinosis with Spontaneous Resolution
- Affiliations
-
- 1Department of Internal Medicine, Korea Cancer Center Hospital, Seoul, Korea. jclee@kcch.re.kr
- KMID: 1518423
- DOI: http://doi.org/10.4046/trd.2007.63.3.294
Abstract
- Pulmonary alveolar proteinosis is a rare disorder that is characterized by the abundant accumulation of surfactant-derived material within the alveolar spaces and distal bronchioles. Although the findings of homogenous ground-glass opacities overlaid by thickened septa, which form a "crazy paving" pattern on high-resolution computed tomography, can assist in making a diagnosis, a lung biopsy is usually required. This disorder has a variable clinical course, from spontaneous resolution to respiratory failure and death. While a whole lung lavage has been the standard treatment since the early 1960s, GM-CSF therapy has been attempted based on the recently suggested pathogenetic mechanism. We report a case of pulmonary alveolar proteinosis that resolved spontaneously after an open lung biopsy.
MeSH Terms
Figure
-
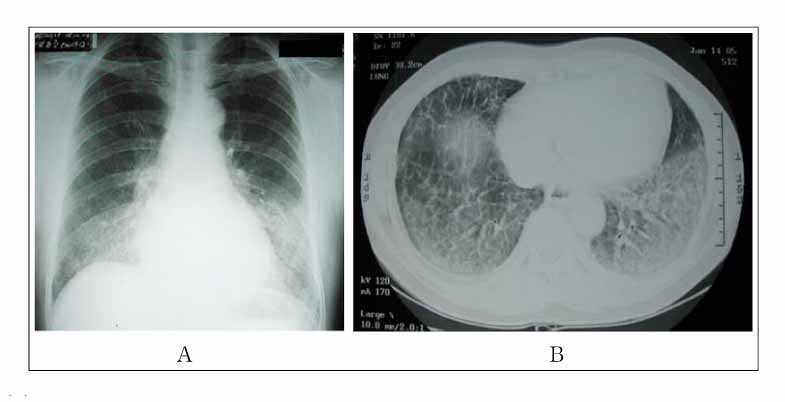
Figure 1 (A) Chest X-ray showing diffuse, patchy and ground-glass opacities on both middle and lower lung field. (B) Diffuse ground glass opacities and airspace consolidations with interlobular septal thickenings on chest CT.
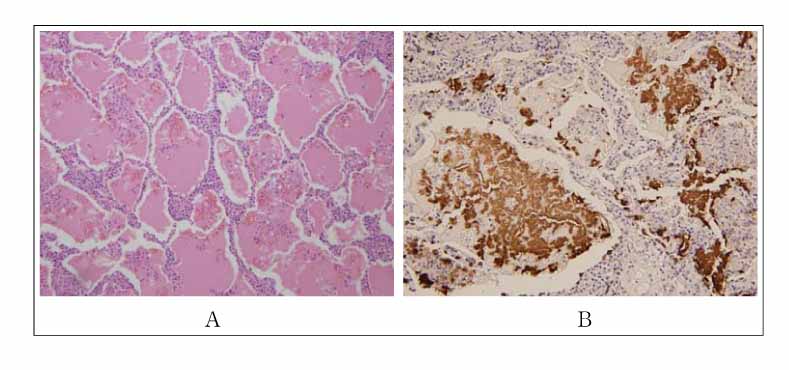
Figure 2 (A) Diffuse eosinophilic materials occupying the alveolar space with relative preservation of the parenchymal architecture on light microscopy (H & E, ×100). Some inflammatory cells were found in the alveolar walls suggesting the possible secondary infection. (B) Abundant materials in alvoelar space were positive on the immunohistochemical staining for surfactant protein A (×200).
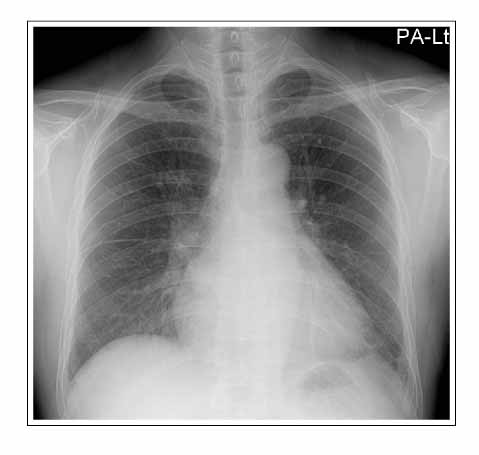
Figure 3 Bilateral patchy and ground-glass opacities completely resolved on a follow-up chest X-ray taken five months after the open lung biopsy.
Reference
-
1. Rosen SH, Castleman B, Liebow AA. Pulmonary alveolar proteinosis. N Engl J Med. 1958. 258:1123–1142.2. Stanley E, Lieschke GJ, Grail D, Metcalf D, Hodgson G, Gall JA, et al. Granulocyte/macrophage colony-stimulating factor-deficient mice show no major perturbation of hematopoiesis but develop a characteristic pulmonary pathology. Proc Natl Acad Sci USA. 1994. 91:5592–5596.3. Trapnell BC, Whitsett JA, Nakata K. Pulmonary alveolar proteinosis. N Engl J Med. 2003. 349:2527–2539.4. Seymour JF, Presneill JJ. Pulmonary alveolar proteinosis: Progress in the first 44 years. Am J Respir Crit Care Med. 2002. 166:215–235.5. Kim G, Lee SJ, Lee HP, Yoo CG, Han SK, Shim YS, et al. The clinical characteristics of pulmonary alveolar proteinosis: experience at Seoul National University Hospital, and review of the literature. J Korean Med Sci. 1999. 14:159–164.6. Seo JH, Bahk JH. Whole Lung Lavage and Extracorporeal Membrane Oxygenation in a Patient with Pulmonary Alveolar Proteinosis and Lung cancer. Korean J Anesthesiol. 2005. 48:549–552.7. Maygarden SJ, Iacocca MV, Funkhouser WK, Novotny DB. Pulmonary alveolar proteinosis: a spectrum of cytologic, histochemical, and ultrastructural findings in bronchoalveolar lavage fluid. Diagn Cytopathol. 2001. 24:389–395.8. Wang BM, Stern EJ, Schmidt RA, Pierson DJ. Diagnosing pulmonary alveolar proteinosis. A review and an update. Chest. 1997. 111:460–466.9. Ioachimescu OC, Kavuru MS. Pulmonary alveolar proteinosis. Chron Respir Dis. 2006. 3:149–159.10. Venkateshiah SB, Yan TD, Bonfield TL, Thomassen MJ, Meziane M, Czich C, et al. An open-label trial of granulocyte macrophage colony stimulating factor therapy for moderate symptomatic pulmonary alveolar proteinosis. Chest. 2006. 130:227–237.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Anesthetic Management for Whole-Lung Lavage in a Patient with Pulmonary Alveolar Proteinosis
- Bilateral Sequential Bronchopulmonary Lavage in One Stage for Recurred Pulmonary Alveolar Proteinosis: A case report
- Anesthetic Management of Lung Lavage in Patient with Pulmonary Alveolar Proteinosis Related to Pneumoconiosis: A case report
- Anesthetic Management for Sequential Bronchoalveolar Lavage in a Patient with Pulmonary Alveolar Proteinosis: A case report
- Bilateral Sequential Bronchopulmonary Lavage for Pulmonary Alveolar Proteinosis
