J Korean Endocr Soc.
2007 Jun;22(3):210-214. 10.3803/jkes.2007.22.3.210.
A Case of Inappropriate Antidiuretic Hormone Syndrome Complicated with Tuberculous Meningitis Refractory to Antituberculosis Drugs
- Affiliations
-
- 1Department of Internal Medicine, College of Medicine, Pochon CHA University, Korea.
- 2Department of Neurosurgery, College of Medicine, Pochon CHA University, Korea.
- KMID: 1512033
- DOI: http://doi.org/10.3803/jkes.2007.22.3.210
Abstract
- Syndrome of inappropriate antidiuretic hormone is the most common cause of hyponatremia in hospitalized patients. It is defined as retention of water, loss of sodium and inappropriately concentrated urine in euvolemic patients with normal renal and adrenal function. A 26-year old male was admitted due to weight loss and fever that he had experienced for the previous 1 month. The chest X-ray and CT scan of lung showed about 2.5x1.2 cm lymph node enlargement at the left hilum and multiple lymph node enlargements. Thoracoscopic biopsy revealed tuberculosis. During treatment with antituberculosis drugs, the serum sodium was 125 mEq/L, the serum osmolality was 263 mOsm/kg, the urine osmolality was 577 mOsm/kg, and the urine sodium concentration was 177 mEq/L. He was treated by fluid restriction and hypertonic saline infusion, but he did not improve. Brain CT scan showed tuberculous meningitis with hydrocephalus. He fully recovered after undergoing ventriculoperitoneal shunt. We report here on a case of inappropriate antidiuretic hormone syndrome complicated by tuberculous meningitis that was refractory to antituberculosis drugs.
MeSH Terms
Figure
-

Fig. 1 Chest x-ray shows ovoid opacity at left suprahilar portion (white arrow).

Fig. 2 Chest CT shows multiple lymph node enlargement at anterior mediastinum and paraaortic portion (Fig. 2A, white arrows), left main bronchus was compressed by lymph node enlargement at left hilum and left lower paratracheal portion extrinsically (Fig. 2B, white arrow).

Fig. 3 Non-contrast brain CT scan shows communicating hydrocephalus. This CT axial image demonstrates dilatation of the lateral ventricles.
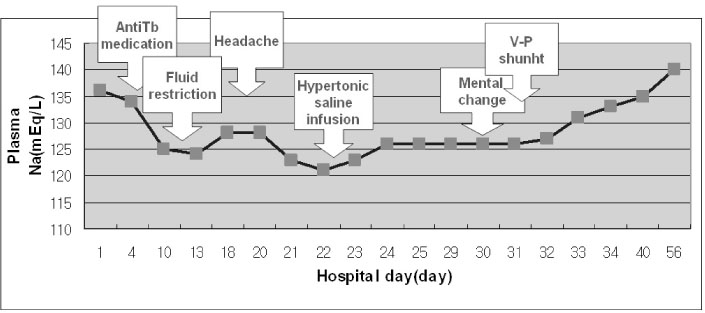
Fig. 4 Plasma sodium concentration according to hospital days. Sodium concentration recovered after the ventriculoperitoneal (V-P) shunt operation.
Reference
-
1. Anderson RJ. Hospital-associated hyponatremia. Kidney Int. 1986. 29:1237–1247.2. Schwartz WB, Bennett W, Curelop S, Bartter FC. A syndrome of renal sodium loss and hyponatremia probably resulting from inappropriate secretion of antidiuretic hormone. Am J Med. 1957. 23:529–542.3. Gary LR. Kasper DL, editor. Disorders of the neurohypophysis. Harrison's Principles of Internal Medicine. 2004. 16th ed. New York: McGraw-Hill;2102.4. Ishikawa S, Kuratomi Y, Saito T. A case of oat cell carcinoma of the lung associated with ectopic production of ADH, neurophysin and ACTH. Endocrinol Jpn. 1980. 27:257–263.5. Kelestimur H, Leach RM, Ward JP, Forsling ML. Vasopressin and oxytocin release during prolonged environmental hypoxia in the rat. Thorax. 1997. 52:84–88.6. Girgis NI, Sultan Y, Farid Z, Mansour MM, Erian MW, Hanna LS, Mateczun AJ. Tuberculous meningitis, Abbassia Fever Hospital-Naval Medical Research Unit No. 3-Cairo, Egypt, from 1976 to 1996. Am J Trop Med Hyg. 1998. 58:28–34.7. Hosoglu S, Geyik MF, Balik I, Aygen B, Erol S, Aygencel TG, Mert A, Saltoglu N, Dokmetas I, Felek S, Sunbul M, Irmak H, Aydin K, Kokoglu OF, Ucmak H, Altindis M, Loeb M. Predictors of outcome in patients with tuberculous meningitis. Int J Tuberc Lung Dis. 2002. 6:64–70.8. Singh BS, Patwari AK, Deb M. Serum sodium and osmolar changes in tuberculous meningitis. Indian Pediatr. 1994. 31:1345–1350.9. Bartter FC, Schwartz WB. The syndrome of inappropriate secretion of antidiuretic hormone. Am J Med. 1967. 42:790–806.10. Renaud LP. Hypothalamic magnocellular neurosecretory neurons: intrinsic membrane properties and synaptic connections. Prog Brain Res. 1994. 100:133–137.11. Vorherr H, Massry SG, Fallet R, Kaplan L, Kleeman CR. Antidiuretic principle in tuberculous lung tissue of a patient with pulmonary tuberculosis and hyponatremia. Ann Intern Med. 1970. 72:383–387.12. DeFronzo RA, Goldberg M, Agus ZS. Normal diluting capacity in hyponatremic patients: reset osmostat or a variant of the syndrome of inappropriate antidiuretic hormone secretion. Ann Intern Med. 1976. 84:538–542.13. Leonard JM, Des Prez RM. Tuberculous meningitis. Infect Dis Clin North Am. 1990. 4:769–787.14. Fong GC, Cheung RT, Ho SL, Lau CS. Brainstem tuberculoma mimicking glioma. Neurology. 1999. 53:1894–1895.15. Verdon R, Chevret S, Laissy JP, Wolff M. Tuberculous meningitis in adults: review of 48 cases. Clin Infect Dis. 1996. 22:982–988.16. Rapoport S, West CD, Brodsky WA. Salt losing conditions; the renal defect in tuberculous meningitis. J Lab Clin Med. 1951. 37:550–561.17. Narotam PK, Kemp M, Buck R, Gouws E, van Dellen JR, Bhoola KD. Hyponatremic natriuretic syndrome in tuberculous meningitis: the probable role of atrial natriuretic peptide. Neurosurgery. 1994. 34:982–988.18. Sakarcan A, Bocchini J Jr. The role of fludrocortisone in a child with cerebral salt wasting. Pediatr Nephrol. 1998. 12:769–771.19. Park CJ, Paik NJ, Lee OJ, Park SH, Byun HW. A case of SIADH with pulmonary tuberculosis and tuberculous meningitis. Tuber Respir Dis. 1978. 25:22–25.20. Song HK, Kim JH, Chung KC, Kim MH. Cranial nerve palsies in adult tuberculosis meningitis. J Clin Neurol. 1989. 7:237–243.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Syndrome of Inappropriate Antidiuretic Hormone Secretion and Pneumomediastinum Complicated by Bougienation in Malignant Esophageal Stricture
- A Case of Severe Drug Fever with Tuberculous Meningitis
- A case of syndrome of inappropriate secretion of antidiuretic hormone associated with paroxetine
- A Case with the Syndrome of Inappropriate Antidiuretic Hormone Associated with Sertraline
- Drug Induced Hyponatremia in the Elderly
