Pseudo-Spontaneous Nystagmus in Lateral Semicircular Canal Benign Paroxysmal Positional Vertigo
- Affiliations
-
- 1Department of Otolaryngology-Head and Neck Surgery, Hallym University College of Medicine, Anyang, Korea. hyojlee@hallym.ac.kr
- KMID: 1489079
- DOI: http://doi.org/10.3342/ceo.2012.5.4.201
Abstract
OBJECTIVES
Spontaneous nystagmus, which has been considered a typical sign of acute vestibulopathy, has recently been reported in benign paroxysmal positional vertigo involving the lateral semicircular canals (LC-BPPV) without unilateral vestibulopathy (pseudo-spontaneous nystagmus, PSN), but research about its clinical application is still limited. Here we investigate the frequency and characteristics of PSN in LC-BPPV patients, and estimate its prognostic value.
METHODS
For 95 patients with LC-BPPV, we examined nystagmus in the sitting position in the clinic with video goggles. Patients were categorized as PSN or non-PSN, according to presence of horizontal nystagmus in the sitting position at diagnosis. The duration of vertiginous symptoms before diagnosis and the duration of treatment were compared between the two groups. The results of video-nystagmography test were reviewed when available.
RESULTS
PSN was examined in 16 (16.8%) patients, all of whose symptoms disappeared immediately after successful repositioning therapy. While the duration of symptoms did not differ statistically between groups (P=0.481), the duration of treatment in the PSN group was significantly longer than in the non-PSN group (P<0.001).
CONCLUSION
We conclude that the presence of spontaneous nystagmus in the sitting position does not preclude a diagnosis of LC-BPPV without unilateral vestibulopathy. PSN was related to a poor outcome of LC-BPPV in this study.
Figure
-
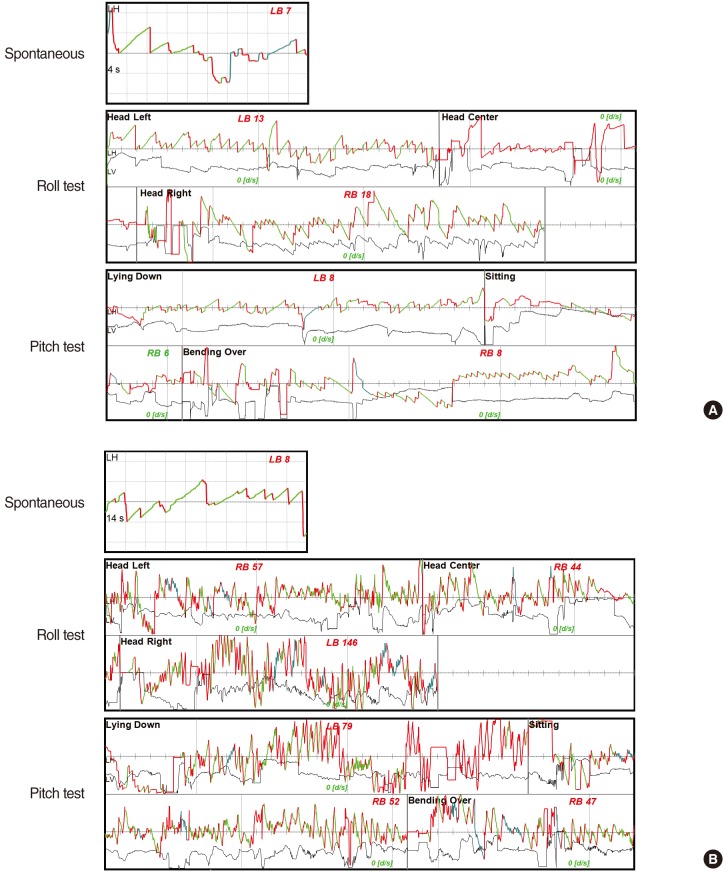
Fig. 1 Video nystagmograms showing pseudo-spontaneous nystagmus (PSN) and positional nystagmus in representative cases of LC-BPPV. (A) A case of geotropic type involving the right ear. Left-beating PSN (7 degree/second) is recorded. In supine roll test, geotropic nystagmus is recorded in the head right (18 degree/second, directing to the right side) and head left (13 degree/second, direction to the left side) position. When the positional test is performed in the pitch plane, lying-down nystagmus and bending-over nystagmus are directed to the same (left-beating, 8 degree/second) and to the opposite direction (right-beating, 8 degree/second) as the PSN, respectively. (B) A case of apogeotropic type involving the left ear. Left-beating PSN (8 degree/second) is recorded. Apogeotropic type nystagmus is examined in the supine roll test (left-beating, 146 degree/second with the head turned to the right; right-beating, 57 degree/second to the left). In the pitch plane, the direction of evoked nystagmus was the same as the direction for PSN in the lying down position (left-beating, 79 degree/second), and to the opposite direction in the bending over position (right-beating, 47 degree/second). LC-BPPV, benign paroxysmal positional vertigo involving the lateral semicircular canal; LH, horizontal component of nystagmus measured on the left eye; LB, nystagmus of which fast component directing to the left side of the patient; RB, nystagmus of which fast component directing to the right side of the patient.
Reference
-
1. Hamid M. Medical management of common peripheral vestibular diseases. Curr Opin Otolaryngol Head Neck Surg. 2010; 10. 18(5):407–412. PMID: 20827085.
Article2. Asprella Libonati G. Diagnostic and treatment strategy of lateral semicircular canal canalolithiasis. Acta Otorhinolaryngol Ital. 2005; 10. 25(5):277–283. PMID: 16602326.3. Califano L, Melillo MG, Mazzone S, Vassallo A. "Secondary signs of lateralization" in apogeotropic lateral canalolithiasis. Acta Otorhinolaryngol Ital. 2010; 4. 30(2):78–86. PMID: 20559477.4. Asprella-Libonati G. Pseudo-spontaneous nystagmus: a new sign to diagnose the affected side in lateral semicircular canal benign paroxysmal positional vertigo. Acta Otorhinolaryngol Ital. 2008; 4. 28(2):73–78. PMID: 18669071.5. Epley JM. Human experience with canalith repositioning maneuvers. Ann N Y Acad Sci. 2001; 10. 942:179–191. PMID: 11710460.
Article6. Bisdorff AR, Debatisse D. Localizing signs in positional vertigo due to lateral canal cupulolithiasis. Neurology. 2001; 9. 57(6):1085–1088. PMID: 11571338.
Article7. Koo JW, Moon IJ, Shim WS, Moon SY, Kim JS. Value of lying-down nystagmus in the lateralization of horizontal semicircular canal benign paroxysmal positional vertigo. Otol Neurotol. 2006; 4. 27(3):367–371. PMID: 16639276.
Article8. Choung YH, Shin YR, Kahng H, Park K, Choi SJ. 'Bow and lean test' to determine the affected ear of horizontal canal benign paroxysmal positional vertigo. Laryngoscope. 2006; 10. 116(10):1776–1781. PMID: 17003735.
Article9. von Brevern M, Clarke AH, Lempert T. Continuous vertigo and spontaneous nystagmus due to canalolithiasis of the horizontal canal. Neurology. 2001; 3. 56(5):684–686. PMID: 11245729.
Article10. De Stefano A, Kulamarva G, Citraro L, Neri G, Croce A. Spontaneous nystagmus in benign paroxysmal positional vertigo. Am J Otolaryngol. 2011; May-Jun. 32(3):185–189. PMID: 20392532.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- An Atypical Case of Benign Paroxysmal Positional Vertigo of the Anterior Semicircular Canal
- Direction Changing Positional Nystagmus from Canalolithiasis and Cupulolithiasis of Lateral Semicircular Canal
- A Case of Horizontal Canal Benign Paroxysmal Positional Vertigo
- Pathophysiology of Nystagmus in Benign Paroxysmal Positional Vertigo
- Management of Benign Paroxysmal Positional Vertigo
