Korean J Hematol.
2008 Dec;43(4):268-271. 10.5045/kjh.2008.43.4.268.
Primary Granulocytic Sarcoma with Multiple Organ Involvement
- Affiliations
-
- 1Department of Internal Medicine, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea. jhlee3@amc.seoul.kr
- KMID: 1485087
- DOI: http://doi.org/10.5045/kjh.2008.43.4.268
Abstract
- We report here a case of primary granulocytic sarcoma that involved multiple organs simultaneously and simulated clinical features of lymphoma at initial presentation. A 55 year-old man was referred to our center for the treatment and evaluation of lymphoma, which was diagnosed for nasal and colonic polyps in a local hospital. In our center, brain MR imaging showed multiple soft tissue lesions in brain and the whole body PET demonstrated multiple hypermetabolic lesions. Immunohistochemical staining of biopsy specimen on nasal and colonic polyp showed negativity of all lymphoma markers and positivity of myeloid markers, and final pathologic diagnosis was granulocytic sarcoma. Cytogenetic analysis of malignant cells in CSF showed chromosomal abnormalities of t(16;16)(p13.1;q22). Bilateral bone marrow examination was done with no evidence of abnormal cell infiltration and with normal cytogenetics. Complete remission was induced with 5 cycles of anti-leukemic chemotherapy, intrathecal chemotherapy and whole brain irradiation. However, leukemia relapsed in blood and bone marrow three months after the completion of treatment and the patient died 11.5 months after initial diagnosis of primary granulocytic sarcoma. In conclusion, immune-histochemical staining is necessary to obtain accurate pathologic diagnosis of granulocytic sarcoma. Pathogenetic role of t(16;16) in granulocytic sarcoma should be evaluated and appropriate treatment of primary granulocytic sarcoma should be defined in the future studies.
MeSH Terms
Figure
-
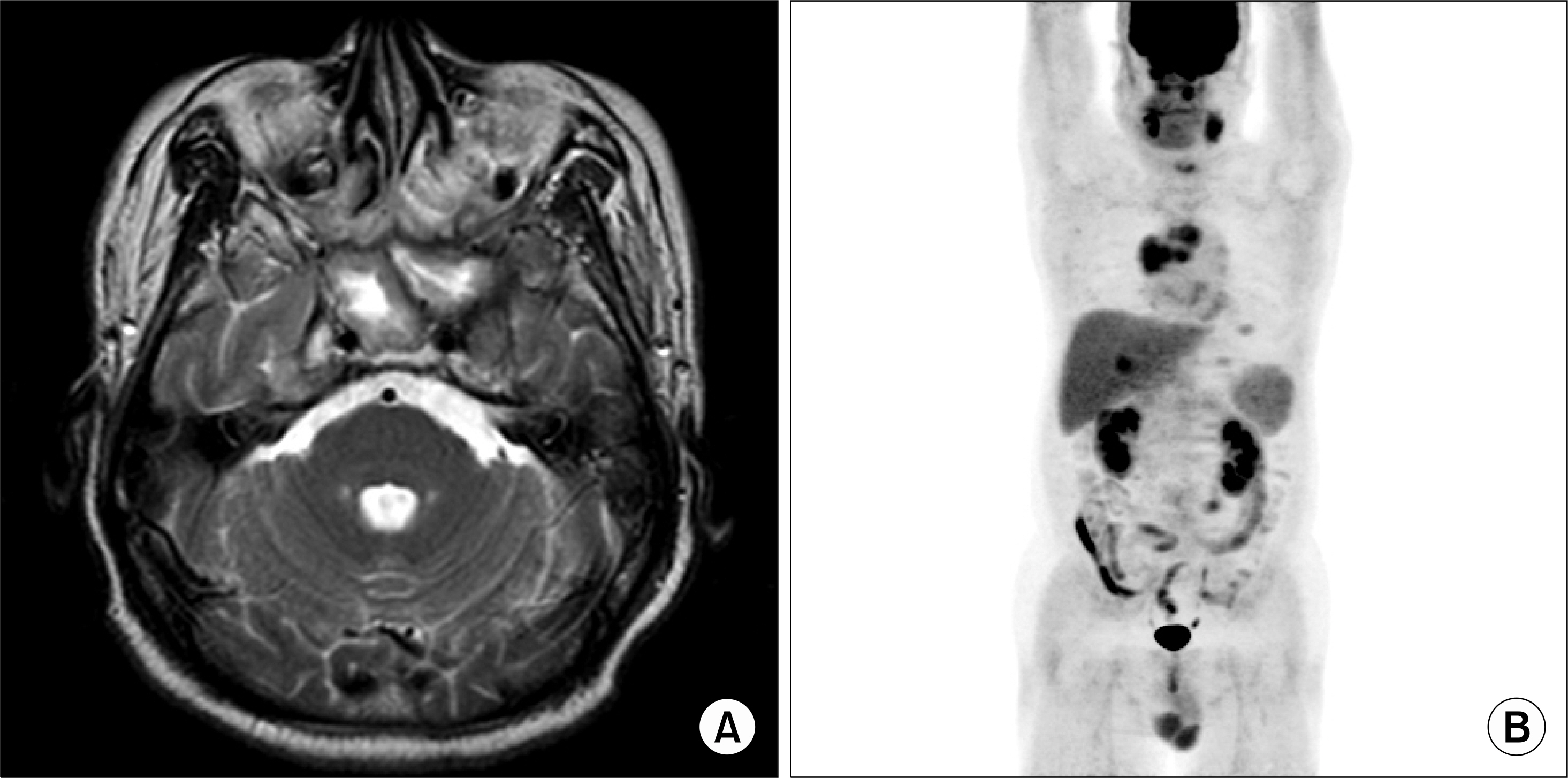
Fig. 1 (A) Brain MR imaging shows soft tissue lesions involving left nasopharynx, left cavernous sinus, Meckel's cave, left infratemporal area, bilateral paranasal sinus, bilateral intraconal and extraconal spaces, and left orbital apex. (B) The whole body PET (F-18 FDG) shows multiple hypermetabolic lesions in left nasopharynx, left skull base, right maxillary sinus, anterior mediastinum, peritoneum, liver, right kidney and multiple lymph node sites (left cervical level Ib, both cervical level II, left cardiophrenic, right paraaortic and left external inguinal).
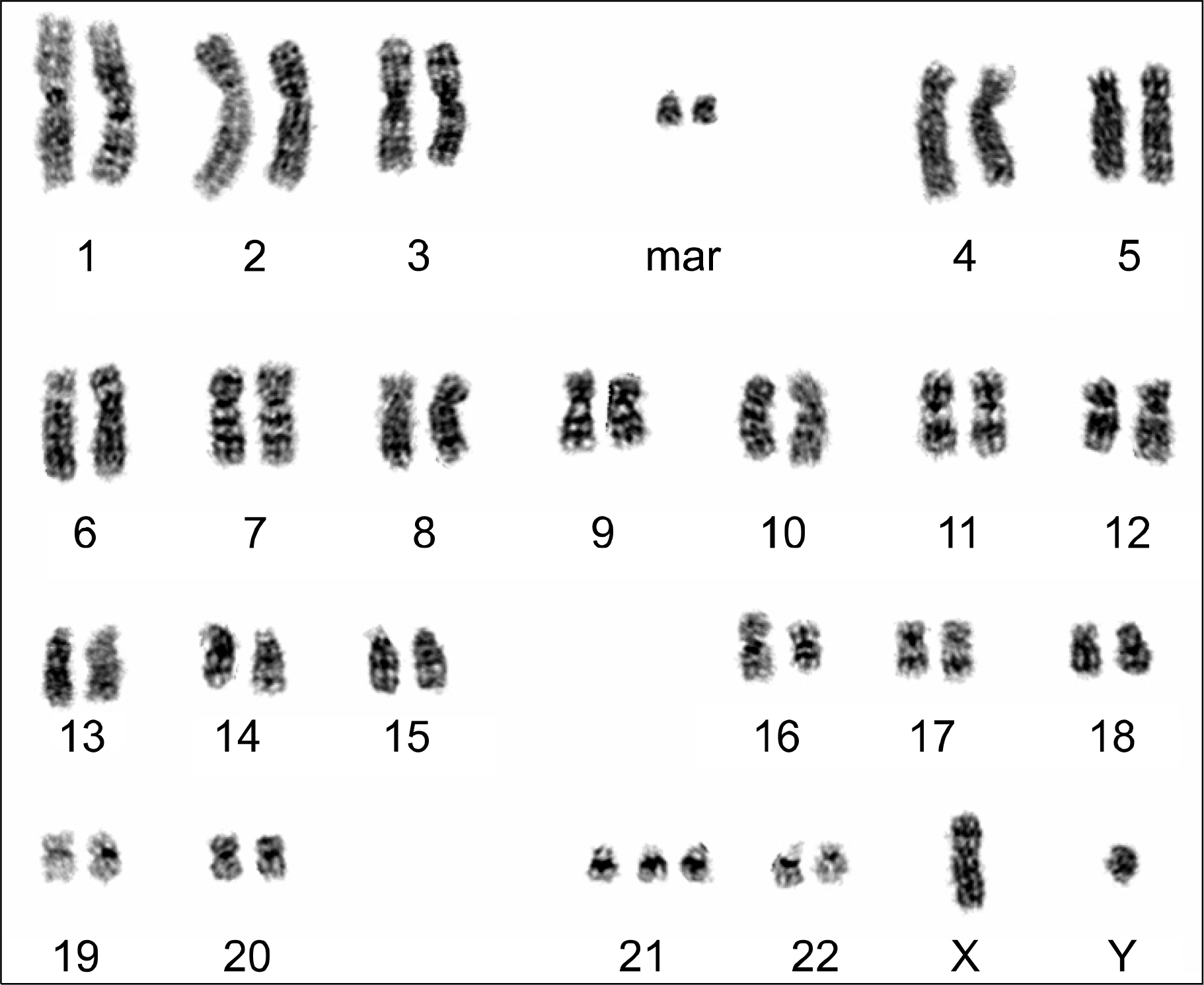
Fig. 2 Cytogenetic analysis was performed using leukemic blasts in the CSF analysis and chromosomal abnormalities of t(16;16)(p13.1;q22), +21, +2mar were noted.
Reference
-
1). Hancock JC., Prchal JT., Bennett JM., Listinsky CM. Trilineage extramedullary myeloid cell tumor in myelodysplastic syndrome. Arch Pathol Lab Med. 1997. 121:520–3.2). Neiman RS., Barcos M., Berard C, et al. Granulocytic sarcoma: a clinicopathologic study of 61 biopsied cases. Cancer. 1981. 48:1426–37.
Article3). Fiegl M., Rieger C., Braess J, et al. Isolated epidural chloroma with translocation t(15;17) successfully treated with chemotherapy and all-trans-retinoic acid. Br J Haematol. 2003. 122:688–9.4). Imrie KR., Kovacs MJ., Selby D, et al. Isolated chloroma: the effect of early antileukemic therapy. Ann Intern Med. 1995. 123:351–3.
Article5). Gittin RG., Scharfman WB., Burkart PT. Granulocytic sarcoma: three unusual patients. Am J Med. 1989. 87:345–7.
Article6). List AF., Gonzalez-Osete G., Kummet T., Doll DC. Granulocytic sarcoma in myelodysplastic syndromes: clinical marker of disease acceleration. Am J Med. 1991. 90:274–6.
Article7). Millot F., Facon T., Kerckaert JP, et al. Unusual recurrence of chronic myelogenous leukemia following bone marrow transplantation. Bone Marrow Transplant. 1991. 7:393–5.8). Kim FS., Rutka JT., Bernstein M., Resch L., Warner E., Pantalony D. Intradural granulocytic sarcoma presenting as a lumbar radiculopathy. Case report. J Neurosurg. 1990. 72:663–7.9). Todd NW Jr., Bowman CA. Acute myelogenous leukemia presenting as atypical mastoiditis with facial paralysis. Int J Pediatr Otorhinolaryngol. 1984. 7:173–7.
Article10). Glossmann JP., Staak JO., Wickenhauser C., Diehl V., Josting A. Extramedullary acute myeloid leukemia (granulocytic sarcoma) with arm paresis, maculopapular exanthema and organ involvement. Leuk Lymphoma. 2003. 44:1619–21.
Article11). Landis DM., Aboulafia DM. Granulocytic sarcoma: an unusual complication of aleukemic myeloid leukemia causing spinal cord compression. A case report and literature review. Leuk Lymphoma. 2003. 44:1753–60.
Article12). Byrd JC., Edenfield WJ., Shields DJ., Dawson NA. Extramedullary myeloid cell tumors in acute non-lymphocytic leukemia: a clinical review. J Clin Oncol. 1995. 13:1800–16.
Article13). Menasce LP., Banerjee SS., Beckett E., Harris M. Extramedullary myeloid tumour (granulocytic sarcoma) is often misdiagnosed: a study of 26 cases. Histopathology. 1999. 34:391–8.
Article14). Mrózek K., Bloomfield CD. Clinical significance of the most common chromosome translocations in adult acute myeloid leukemia. J Natl Cancer Inst Monogr. 2008. 39:52–7.15). Kelly J., Foot NJ., Conneally E, et al. 3'CBFbeta deletion associated with inv(16) in acute myeloid leukemia. Cancer Genet Cytogenet. 2005. 162:122–6.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Extradural Granulocytic Sarcoma of the Thoracic Spine
- Multiple Granulocytic Sarcomas in a Patient with Longstanding Complete Remission of Acute Myelogenous Leukemia
- A Case of Isolated Granulocytic Sarcoma of the Ovary in Nonleukemic Patients
- A case of granulocytic sarcoma of the pancreas and kidney in a patient presenting with jaundice
- Granulocytic Sarcoma in the Leg Mimicking Hemorrhagic Abscess
