A Case of Graves' Disease Presenting with Chorea
- Affiliations
-
- 1Department of Internal Medicine, College of Medicine, Yonsei University, Korea.
- 2Department of Neurology, College of Medicine, Yonsei University, Korea.
- 3Department of Internal Medicine, Dong Rae Bong Seng Hospital, Korea.
- KMID: 1479228
- DOI: http://doi.org/10.3803/jkes.2008.23.5.342
Abstract
- Hyperthyroidism is invariably accompanied by nervous system dysfunction. Specifically, irritability, emotional lability, and hyperkinesia are the signs and symptoms most frequently observed. In rare instances, chorea and/or choreoathetosis are associated with hyperthyroidism. Full evaluation for the etiology of chorea is necessary prior to initiating treatment. We recently encountered a 42-year-old female who initially presented with hyperthyroidism and showed subsequent development of progressive generalized chorea. The patient was diagnosed with chorea secondary to Graves' disease after exclusion of other causes of chorea and improved after the initiation of pulse administration of intravenous methylprednisolone sodium succinate (Solu-medrol(R), 1000 mg for 5 days) and oral antithyroid medication. This treatment strategy resulted in the resolution of involuntary movements. The steroid administration was eventually tapered, and the patient has been maintained on antithyroid and steroid therapy with considerable success since the initiation of treatment.
Keyword
MeSH Terms
Figure
-
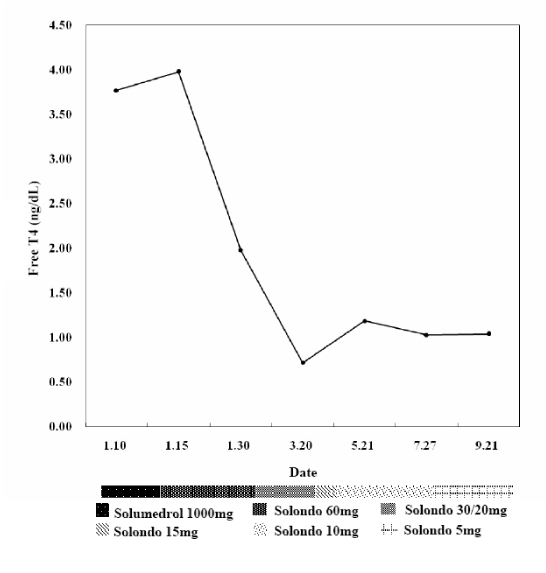
Fig. 1 Serial changes in free T4 thyroid hormone levels (Unit: ng/dL). Axis X is the date that steroid tapering occurred. Axis Y is the level of free T4. Each of the dotted bars below axis X represents the steroid dose. On the day of admission, laboratory tests revealed free T4 levels of 3.77 ng/dL, T3 levels of 273 ng/dL, TSH levels of < 0.01 µIU/mL, and TBII at 51%. The final laboratory tests (September 21st, 2007) revealed normalization with free T4 levels of 1.04 µg/dL, T3 levels of 163 ng/m, TSH levels of 1.25 µIU/mL, and a TBII of 15%. Steroid administration was eventually tapered off to 5 mg daily and PTU has been maintained at 100 mg daily. The patient has been successfully managed with antithyroid and steroid therapy since the initiation of treatment, without recurrence of choreic movement.
Reference
-
1. Smith MA, Brandt J, Shadmehr R. Motor disorder in Huntington's disease begins as a dysfunction in error feedback control. Nature. 2000. 403:544–549.2. Postuma RB, Lang AE. Hemiballism: revisiting a classic disorder. Lancet Neurol. 2003. 2:661–668.3. Janavs JL, Aminoff MJ. Dystonia and chorea in acquired systemic disorders. J Neurol Neurosurg Psychiatry. 1998. 65:436–445.4. Piccolo I, Defanti CA, Soliveri P, Volonte MA, Cislaghi G, Girotti F. Cause and course in a series of patients with sporadic chorea. J Neurol. 2003. 250:429–435.5. Ristic AJ, Svetel M, Dragasevic N, Zarkovic M, Koprivsek K, Kostic VS. Bilateral chorea-ballism associated with hyperthyroidism. Mov Disord. 2004. 19:982–983.6. Yudiarto FL, Muliadi L, Moeljanto D, Hartono B. Neuropsychological findings in hyperthyroid patients. Acta Med Indones. 2006. 38:6–10.7. Jabbari B, Huott AD. Seizures in thyrotoxicosis. Epilepsia. 1980. 21:91–96.8. Ratanakorn D, Vejjajiva A. Long-term follow-up of myasthenia gravis patients with hyperthyroidism. Acta Neurol Scand. 2002. 106:93–98.9. Ober KP. Thyrotoxic periodic paralysis in the United States. Report of 7 cases and review of the literature. Medicine (Baltimore). 1992. 71:109–120.10. Duyff RF, Van den Bosch J, Laman DM, van Loon BJ, Linssen WH. Neuromuscular findings in thyroid dysfunction: a prospective clinical and electrodiagnostic study. J Neurol Neurosurg Psychiatry. 2000. 68:750–755.11. Baba M, Terada A, Hishida R, Matsunaga M, Kawabe Y, Takebe K. Persistent hemichorea associated with thyrotoxicosis. Intern Med. 1992. 31:1144–1146.12. Pozzan GB, Battistella PA, Rigon F, Zancan L, Casara GL, Pellegrino PA, Zacchello F. Hyperthyroid-induced chorea in an adolescent girl. Brain Dev. 1992. 14:126–127.13. Javaid A, Hilton DD. Persistent chorea as a manifestation of thyrotoxicosis. Postgrad Med J. 1988. 64:789–790.14. Blindauer K. Myoclonus and its disorders. Neurol Clin. 2001. 19:723–734. viii.15. Taurin G, Golfier V, Pinel JF, Deburghgraeve V, Poirier JY, Edan G, Verin M. Choreic syndrome due to Hashimoto's encephalopathy. Mov Disord. 2002. 17:1091–1092.16. Canton A, de Fabregas O, Tintore M, Mesa J, Codina A, Simo R. Encephalopathy associated to autoimmune thyroid disease: a more appropriate term for an underestimated condition? . J Neurol Sci. 2000. 176:65–69.17. Seo SW, Lee BI, Lee JD, Park SA, Kim KS, Kim SH, Yun MJ. Thyrotoxic autoimmune encephalopathy: a repeat positron emission tomography study. J Neurol Neurosurg Psychiatry. 2003. 74:504–506.18. Utku U, Asil T, Celik Y, Tucer D. Reversible MR angiographic findings in a patient with autoimmune Graves disease. AJNR Am J Neuroradiol. 2004. 25:1541–1543.19. Isaacs JD, Rakshi J, Baker R, Brooks DJ, Warrens AN. Chorea associated with thyroxine replacement therapy. Mov Disord. 2005. 20:1656–1657.20. Cretel E, Amoura Z, Piette JC. Hyperthyroidism-associated chorea. Lancet. 1998. 352:239.
