Korean J Hepatobiliary Pancreat Surg.
2013 Aug;17(3):126-130. 10.14701/kjhbps.2013.17.3.126.
Duodenum-preserving pancreatic head resection in benign and low-grade malignant pancreatic tumors
- Affiliations
-
- 1Department of Surgery, Severance Hospital, Yonsei University College of Medicine, Seoul, Korea. kskim88@yuhs.ac
- 2Department of Surgery, Yongin Severance Hospital, Yonsei University College of Medicine, Yongin, Korea.
- 3Department of Surgery, Wonju Severance Christian Hospital, Yonsei University Wonju College of Medicine, Wonju, Korea.
- 4Department of Pathology, Severance Hospital, Yonsei University College of Medicine, Seoul, Korea.
- 5Department of Internal Medicine, Severance Hospital, Yonsei University College of Medicine, Seoul, Korea.
- KMID: 1472528
- DOI: http://doi.org/10.14701/kjhbps.2013.17.3.126
Abstract
- BACKGROUNDS/AIMS
With development of imaging techniques, pancreatic tumors are being diagnosed more frequently. Applying the standard surgical procedures for pancreatic head tumors, such as pancreaticoduodenectomy and pylorus-preserving pancreaticoduodenectomy may seem too extensive for benign or low-grade malignant pancreas head tumors. Duodenum-preserving pancreatic head resection (DPPHR) has been safely performed in patients with chronic pancreatitis. Recently, DPPHR has been used as a limited surgical procedure to remove benign or low-grade malignant pancreatic head lesions. This study is aimed to evaluate the results of DPPHR in benign or low-grade malignant tumors.
METHODS
Between 2004 and 2012, six patients underwent DPPHR due to benign or low-grade malignant pancreas tumor. We performed this retrospective analysis based on the medical records.
RESULTS
Five of six patients were diagnosed as intraductal papillary mucinous neoplasms. Remaining one patient was diagnosed as solid pseudopapillary neoplasm. The median age of patients was 60.3 (27-75) years, and the median follow-up period was 24 months. The operation time, blood loss and length of stay were 442.5 minutes, 680 ml and 19.2 days, respectively. There was no mortality. Five patients experienced complications including 1 delayed gastric empting, 2 bile duct strictures, 1 pancreatic fistula and 1 duodenal stricture. No recurrence or metastasis was found during follow-up.
CONCLUSIONS
In benign and low-grade malignant lesions of pancreatic head, DPPHR could be alternative to traditional surgery. For applying DPPHR in pancreas tumor, a thorough preoperative examination and utilization of frozen section for sufficient resection margin are required.
MeSH Terms
Figure
-
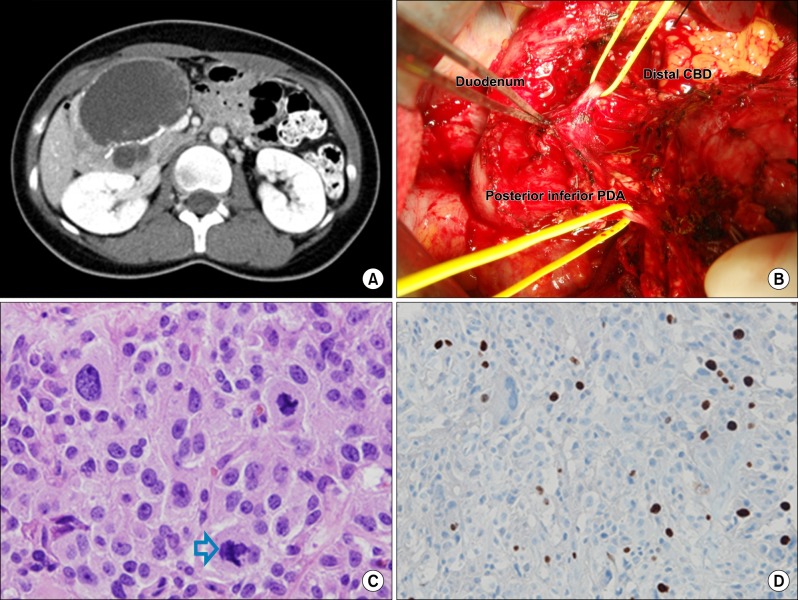
Fig. 1 A case of solid pseudopapillary neoplasm. (A) A 10 cm-sized, septated, cystic mass in the pancreas head. (B) Duodenum, distal common bile duct and posterior inferior pancreaticoduodenal artery (PDA) were preserved during the duodenum-preserving pancreatic head resection. (C) Atypical mitosis; Tripolar mitosis (arrow) (H-E, ×400). (D) β-catenin was found to be positive for nuclear pattern (×400).
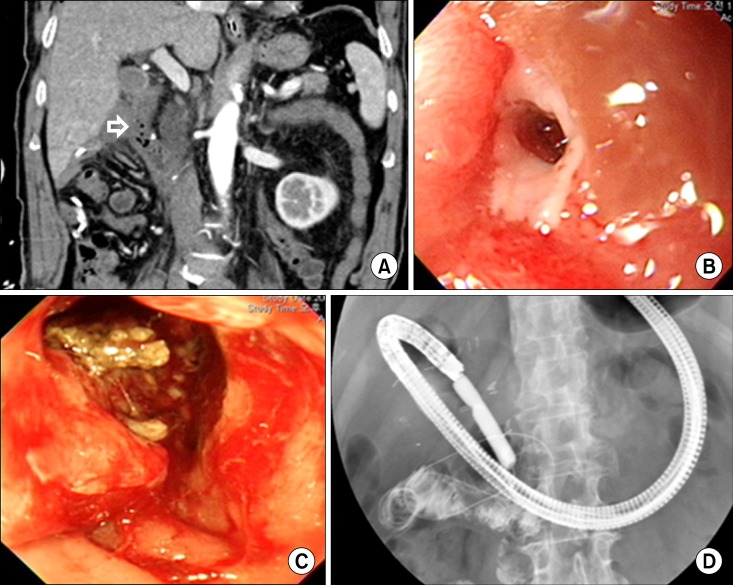
Fig. 2 Complications presenting duodenal stricture. (A) Ischemic change at the duodenal 2nd portion (arrow). (B) Huge ulcero-infiltrative lesion at duodenum. (C) Duodenal stricture. (D) Pneumatic balloon dilatation of the duodenum.
Reference
-
1. Klöppel G, Kosmahl M. Cystic lesions and neoplasms of the pancreas. The features are becoming clearer. Pancreatology. 2001; 1:648–655. PMID: 12120249.2. Ferrone CR, Correa-Gallego C, Warshaw AL, et al. Current trends in pancreatic cystic neoplasms. Arch Surg. 2009; 144:448–454. PMID: 19451487.
Article3. Salvia R, Malleo G, Marchegiani G, et al. Pancreatic resections for cystic neoplasms: from the surgeon's presumption to the pathologist's reality. Surgery. 2012; 152(3 Suppl 1):S135–S142. PMID: 22766364.
Article4. Beger HG, Krautzberger W, Bittner R, et al. Duodenum-preserving resection of the head of the pancreas in patients with severe chronic pancreatitis. Surgery. 1985; 97:467–473. PMID: 3983823.5. Beger HG, Gansauge F, Siech M, et al. Duodenum-preserving total pancreatic head resection for cystic neoplastic lesions in the head of the pancreas. J Hepatobiliary Pancreat Surg. 2008; 15:149–156. PMID: 18392707.
Article6. Möbius C, Max D, Uhlmann D, et al. Five-year follow-up of a prospective non-randomised study comparing duodenum-preserving pancreatic head resection with classic Whipple procedure in the treatment of chronic pancreatitis. Langenbecks Arch Surg. 2007; 392:359–364. PMID: 17375317.
Article7. Pedrazzoli S, Canton SA, Sperti C. Duodenum-preserving versus pylorus-preserving pancreatic head resection for benign and premalignant lesions. J Hepatobiliary Pancreat Sci. 2011; 18:94–102. PMID: 20694480.
Article8. Takada T, Yasuda H, Amano H, et al. A duodenum-preserving and bile duct-preserving total pancreatic head resection with associated pancreatic duct-to-duct anastomosis. J Gastrointest Surg. 2004; 8:220–224. PMID: 15036200.
Article9. Takada T, Yasuda H, Amano H, et al. A duodenum-preserving and bile duct-preserving total pancreatic head resection with associated pancreatic duct-to-duct anastomosis. J Gastrointest Surg. 2004; 8:220–224. PMID: 15036200.
Article10. Takada T, Yasuda H, Uchiyama K, et al. Duodenum-preserving pancreatoduodenostomy. A new technique for complete excision of the head of the pancreas with preservation of biliary and alimentary integrity. Hepatogastroenterology. 1993; 40:356–359. PMID: 8406305.11. Miyakawa S, Horiguchi A, Mizuno K, et al. Preservation of arterial arcades during duodenum-preserving total pancreatic head resection for intraductal papillary tumor. Hepatogastroenterology. 2003; 50:993–997. PMID: 12845965.12. Horiguchi A, Miyakawa S, Ishihara S, et al. Surgical design and outcome of duodenum-preserving pancreatic head resection for benign or low-grade malignant tumors. J Hepatobiliary Pancreat Sci. 2010; 17:792–797. PMID: 19894017.
Article13. Beger HG, Rau BM, Gansauge F, et al. Duodenum-preserving total pancreatic head resection for cystic neoplasm: a limited but cancer-preventive procedure. Langenbecks Arch Surg. 2008; 393:589–598. PMID: 18379818.14. Tanaka M, Chari S, Adsay V, et al. International consensus guidelines for management ofintraductal papillary mucinous neoplasms and mucinous cystic neoplasms of the pancreas. Pancreatology. 2006; 6:17–32. PMID: 16327281.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Duodenum-preserving Pancreatic Head Resection for Benign Pancreatic Head Lesion
- Clinical Efficacy of Organ-Preserving Pancreatectomy for Benign or Low-Grade Malignant Potential Lesion
- Bile duct preserving pancreatic head resection (BDPPHR): Can we conclusively define the extent of head resection in surgery for chronic pancreatitis?
- Duodenum-preserving pancreatic head resection
- Pancreatic Head Resection with Segmental Duodenectomy
