A Case of Graves' Disease with Pancytopenia
- Affiliations
-
- 1Department of Internal Medicine, Eulji University School of Medicine, Daejeon, Korea.
- 2Department of Labolatory Medicine, Eulji University School of Medicine, Daejeon, Korea.
- KMID: 1468547
- DOI: http://doi.org/10.3803/jkes.2009.24.4.272
Abstract
- Hematological disorders, and especially single lineage abnormalities, have been described in patients suffering with thyrotoxicosis, but pancytopenia is a rare complication of thyrotoxicosis. Pancytopenia with thyrotoxicosis has been reported to be totally reversible with antithyroid drug treatment. We experienced a case with pancytopenia associated with Graves' disease in a 57-year-old woman who had no specific cause of pancytopenia. She presented with dyspnea and palpitation. The laboratory findings revealed thyrotoxicosis and pancytopenia. Increased radioisotope uptake was seen on the thyroid scan and normal cellularity and maturation were found in the bone marrow aspiration biopsy. Based on these findings, she was diagnosed as suffering from Gravesyendisease with pancytopenia. After treatment with propylthiouracil, the blood cell counts were restored to normal as the patient achieved a euthyroid state. We report here on a case of Graves' disease that was complicated by pancytopenia, and all this was normalized after treatment for hyperthyroidism.
Keyword
MeSH Terms
Figure
-
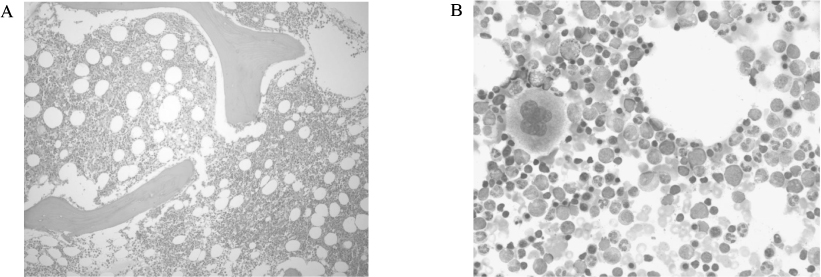
Fig. 1 A. Bone marrow biopsy (H&E stain, ×100). Bone marrow biopsy shows normal cellularity. B. Bone marrow aspiration smear (Wright-Giemsa stain, ×400). Bone marrow aspiration smear shows normal hematopoiesis without abnormal cell infiltration.

Fig. 2 A. Chest PA. Chest PA shows cardiomegaly and multiple calcified nodules and fibrosis on both upper lobes representing sequelae of old pulmonary tuberculosis. B. Abdomen CT scan. Abdomen CT scan does not show splenomegaly.

Fig. 3 Thyroid scan. Thyroid scan shows asymmetric thyroid enlargement and heterogeneously increased radioisotope uptake.
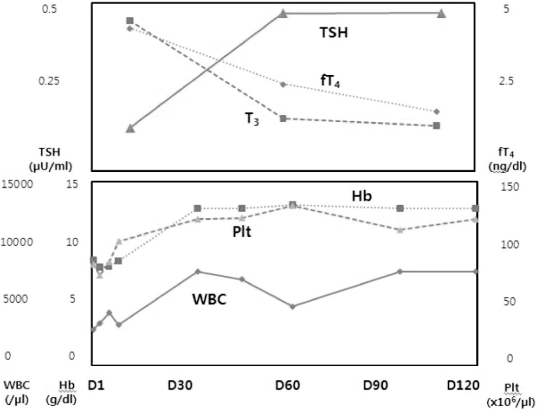
Fig. 4 Clinical course. Antihyperthyroid therapy (PTU 300 mg daily p.o.) was initiated at the time of diagnosis of Graves disease. T3 and fT4 concentration were slowly normalized with restoration of pancytopenia for 3 months. FT4, free T4; T3, total T3; TSH, thyroid stimulating hormone; WBC, white blood cell; Hb, hemoglobin, Plt: platelet.
Reference
-
1. Soeki T, Tamura Y, Kondo N, Shinohara H, Tanaka H, Bando K, Fukuda N. A case of thyrotoxicosis with pancytopenia. Endocr J. 2001. 48:385–389.2. Lima CS, Zantut Wittmann DE, Castro V, Tambascia MA, Lorand-Metze I, Saad ST, Costa FF. Pancytopenia in untreated patient with Graves' disease. Thyroid. 2006. 16:403–409.3. Akoum R, Michel S, Wafic T, Emile B, Marwan M, Khaled H, Gerard A. Myelodysplastic syndrome and pancytopenia responding to treatment of hyperthyroidism: peripheral blood and bone marrow analysis before and after antihormonal treatment. J Cancer Res Ther. 2007. 3:43–46.4. Lee JH, Lee J, Sung SH, Bae SH, Kim SG, Oh HK. A case of methimazole-induced pancytopenia: successful treatment with recombinant human granulocyte colony-stimulating factor. J Korean Soc Endocrinol. 2006. 21:548–551.5. Breier DV, Rendo P, Gonzalez J, Shilton G, Stivel M, Goldztein S. Massive plasmocytosis due to methimazole-induced bone marrow toxicity. Am J Hematol. 2001. 67:259–261.6. Biswas N, Ahn YH, Goldman JM, Schwartz JM. Aplastic anemia associated with antithyroid drugs. Am J Med Sci. 1991. 301:190–194.7. Das KC, Mukherjee M, Sarkar TK, Dash RJ, Rastogi GK. Erythropoiesis and erythropoietin in hypo- and hyperthyroidism. J Clin Endocrinol Metab. 1975. 40:211–220.8. Boitard C, Anciaux-Lespine ML, Eugene C, Quevauvilliers J. Anaemia and microcytosis during thyrotoxicosis. Physiopathological discussion. 36 cases (author's transl). Nouv Presse Med. 1979. 8:499–502.9. Macaron CI, Macaron ZG. Increased serum ferritin levels in hyperthyroidism. Ann Intern Med. 1982. 96:617–618.10. Kuhn JM, Rieu M, Wolf LM, Courtois H, Bricaire H, Luton JP. Hematologic repercussions of disorders of thyroid secretion. Presse Med. 1984. 13:421–425.11. Burns RW, Burns TW. Pancytopenia due to vitamin B12 deficiency associated with Graves' disease. Mo Med. 1996. 93:368–372.12. Lahtinen R. Sideroblast and haemosiderin in thyrotoxicosis. Scand J Haematol. 1980. 25:237–243.13. Adrouny A, Sandler RM, Carmel R. Variable presentation of thrombocytopenia in Graves' disease. Arch Intern Med. 1982. 142:1460–1464.14. Panzer S, Haubenstock A, Minar E. Platelets in hyperthyroidism. Studies on platelet count, mean platelet volume, 111-indium-labeled platelet kinetics, and platelet-associated immunoglobulins G and M. J Clin Endoclinol Metab. 1990. 70:491–496.15. Hymes K, Blum M, Lackner H, Karpatkin S. Easy bruising, thrombocytopenia, and elevated platelet immunoglobulin G in Graves' disease and Hashimoto's thyroiditis. Ann Intern Med. 1981. 94:27–30.16. Kitao T, Takiguchi T, Kawamura H, Miyabo S, Hattori K. Basedow's disease complicated by idiopathic thrombocytopenic purpura. A case report. Nippon Naika Gakkai Zasshi. 1973. 62:380–383.
