Tuberc Respir Dis.
2011 Mar;70(3):257-260. 10.4046/trd.2011.70.3.257.
A Case of Pulmonary Fibrosis with Microscopic Polyangiitis
- Affiliations
-
- 1Department of Pulmonary and Critical Care Medicine, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea. skysong3@hanmail.net
- 2Department of Diagnostic Pathology, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea.
- KMID: 1442857
- DOI: http://doi.org/10.4046/trd.2011.70.3.257
Abstract
- A 65-year-old woman was admitted due to poor oral intake and a dry cough over the previous 3 months. The physical examination was remarkable for bibasilar crackles, and plain chest radiography showed reticulation in both lower lung fields. A pulmonary function test demonstrated a restrictive pattern with a reduced diffusing capacity of the lung for carbon monoxide. High resolution computed tomography showed reticulation and honey-combing in both peripheral lung zones, which was consistent with usual interstitial pneumonia pattern. Her skin showed livedo reticularis. The erythrocyte sedimentation rate and C-reactive protein level were elevated, and hematuria was noted on urinary analysis. A serologic test for auto-antibodies showed seropositivity for Myeloperoxidase-Anti-neutrophil cytoplasmic antibody (MPO-ANCA). A kidney biopsy was performed and showed focal segmental glomerulosclerosis. She was diagnosed as having pulmonary fibrosis with microscopic polyangiitis (MPA) and treated with high dose steroids. Here we report a case of pulmonary fibrosis coexistent with microscopic polyangiitis.
MeSH Terms
-
Aged
Antibodies, Antineutrophil Cytoplasmic
Biopsy
Blood Sedimentation
C-Reactive Protein
Carbon Monoxide
Cough
Cytoplasm
Female
Glomerulosclerosis, Focal Segmental
Hematuria
Humans
Idiopathic Pulmonary Fibrosis
Kidney
Livedo Reticularis
Lung
Microscopic Polyangiitis
Physical Examination
Pulmonary Fibrosis
Respiratory Function Tests
Respiratory Sounds
Serologic Tests
Skin
Steroids
Thorax
Antibodies, Antineutrophil Cytoplasmic
C-Reactive Protein
Carbon Monoxide
Glomerulosclerosis, Focal Segmental
Steroids
Figure
-

Figure 1 Chest PA shows coarse reticular opacities in both peripheral lung zone.

Figure 2 High-resolution CT shows reticular opacity and honey-combing in both peripheral lung zone. CT: computer tomography.

Figure 3 Medium sized vessel wall shows fibrinoid necrosis (H&E, ×200).
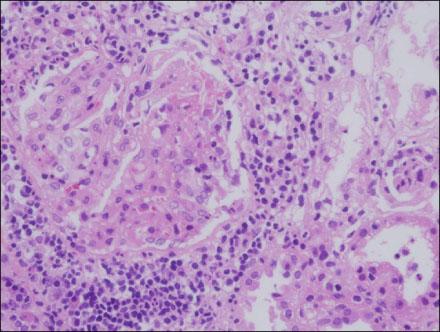
Figure 4 Glomerulus shows focal fibrinoidnecrosis and interstitial inflammatory cell infiltration are observed (H&E, ×200).
Reference
-
1. Collins CE, Quismorio FP Jr. Pulmonary involvement in microscopic polyangiitis. Curr Opin Pulm Med. 2005. 11:447–451.2. Guillevin L, Durand-Gasselin B, Cevallos R, Gayraud M, Lhote F, Callard P, et al. Microscopic polyangiitis: clinical and laboratory findings in eighty-five patients. Arthritis Rheum. 1999. 42:421–430.3. Schwarz MI, Brown KK. Small vessel vasculitis of the lung. Thorax. 2000. 55:502–510.4. Foulon G, Delaval P, Valeyre D, Wallaert B, Debray MP, Brauner M, et al. ANCA-associated lung fibrosis: analysis of 17 patients. Respir Med. 2008. 102:1392–1398.5. Davson J, Ball J, Platt R. The kidney in periarteritis nodosa. Q J Med. 1948. 17:175–202.6. Jennette JC, Thomas DB, Falk RJ. Microscopic polyangiitis (microscopic polyarteritis). Semin Diagn Pathol. 2001. 18:3–13.7. Gallagher H, Kwan JT, Jayne DR. Pulmonary renal syndrome: a 4-year, single-center experience. Am J Kidney Dis. 2002. 39:42–47.8. Eschun GM, Mink SN, Sharma S. Pulmonary interstitial fibrosis as a presenting manifestation in perinuclear antineutrophilic cytoplasmic antibody microscopic polyangiitis. Chest. 2003. 123:297–301.9. Mansi IA, Opran A, Sondhi D, Ayinla R, Rosner F. Microscopic polyangiitis presenting as idiopathic pulmonary fibrosis: is anti-neutrophilic cytoplasmic antibody testing indicated. Am J Med Sci. 2001. 321:201–202.10. Homma S, Matsushita H, Nakata K. Pulmonary fibrosis in myeloperoxidase antineutrophil cytoplasmic antibody-associated vasculitides. Respirology. 2004. 9:190–196.11. Cambridge G, Williams M, Leaker B, Corbett M, Smith CR. Anti-myeloperoxidase antibodies in patients with rheumatoid arthritis: prevalence, clinical correlates, and IgG subclass. Ann Rheum Dis. 1994. 53:24–29.12. Braun MG, Csernok E, Schmitt WH, Gross WL. Incidence, target antigens, and clinical implications of antineutrophil cytoplasmic antibodies in rheumatoid arthritis. J Rheumatol. 1996. 23:826–830.13. Hahn HS, Hwang JK, Jung HS, Song SH, Joo KW, Park GY, et al. Two Cases of Microscopic Polyangiitis with Honeycomb Lung. Tuberc Respir Dis. 2002. 52:550–556.14. Hervier B, Pagnoux C, Agard C, Haroche J, Amoura Z, Guillevin L, et al. Pulmonary fibrosis associated with ANCA-positive vasculitides. Retrospective study of 12 cases and review of the literature. Ann Rheum Dis. 2009. 68:404–407.15. Haegens A, van der Vliet A, Butnor KJ, Heintz N, Taatjes D, Hemenway D, et al. Asbestos-induced lung inflammation and epithelial cell proliferation are altered in myeloperoxidase-null mice. Cancer Res. 2005. 65:9670–9677.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Two Cases of Microscopic Polyangiitis with Honeycomb Lung
- A Case of Microscopic Polyangiitis
- Interstitial Lung Disease and Diffuse Alveolar Hemorrhage, the Two Key Pulmonary Manifestations in Microscopic Polyangiitis
- A Case of Microscopic Polyangiitis Presented as Pleural Effusion
- Two Cases of Microscopic Polyangiitis
