A Case of Microscopic Polyangiitis Presented as Pleural Effusion
- Affiliations
-
- 1Department of Internal Medicine, Bucheon St. Mary's Hospital, The Catholic University of Korea College of Medicine, Bucheon, Korea. kyh30med@catholic.ac.kr
- 2Department of Pathology, Bucheon St. Mary's Hospital, The Catholic University of Korea College of Medicine, Bucheon, Korea.
Abstract
- Microscopic polyangiitis is a necrotizing vasculitis, characterized by inflammation of small vessels (capillaries, venules, and arterioles) with few or no immune deposits. The kidneys are the most commonly affected organs and are involved in 90% of patients, whereas pulmonary involvement occurs in a minority of cases (10% to 30%). In cases of lung disease, diffuse alveolar hemorrhage with pulmonary capillaritis is the most common manifestation. Microscopic polyangiitis is strongly associated with antineutrophil cytoplasmic autoantibody, which is a useful diagnostic serological marker. We report a case of microscopic polyangiitis presented as pleural effusion in a 67-year-old female. Pleural effusions have been reported in some cases previously, but the number of cases were small and their characteristics have not been well described. This report describes characteristic findings of pleural fluid and its histological features in a case of microscopic polyangiitis.
MeSH Terms
Figure
-

Figure 1 Petechiae on the right lower extremity is noted.

Figure 2 Initial chest X-ray shows right pleural effusion (A) and shifting of the right pleural effusion in the right decubitus view (B).

Figure 3 Contrast enhanced CT scan shows right pleural effusion and parietal pleural thickening. CT: computed tomography.

Figure 4 Extravasation of red blood cell (arrow) and perivascular mild mononuclear cell infiltration are found in skin biopsy (H&E stain, ×200).

Figure 5 (A) An interlobular artery shows fibrinoid necrosis (arrow) with perivascular mononuclear cell infiltration (H&E stain, ×200). (B) Celluar crescents (arrow) are found in glomeruli (PAS stain, ×400).
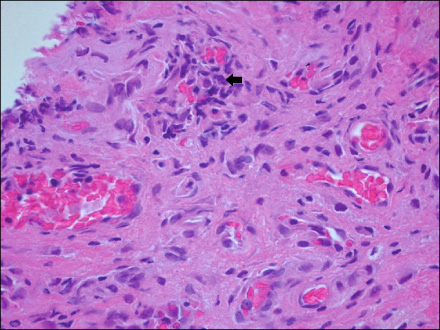
Figure 6 The vascular walls are infiltrated by lymphocytes (arrow) in pleural biopsy (H&E stain, ×200).

Figure 7 One month after steroid therapy, chest X-ray shows a regression of previously noted right pleural effusion.
Reference
-
1. Jennette JC, Falk RJ, Andrassy K, Bacon PA, Churg J, Gross WL, et al. Nomenclature of systemic vasculitides. Proposal of an international consensus conference. Arthritis Rheum. 1994. 37:187–192.2. Watts R, Scott DG. Hochberg MC, Silman AJ, Smolen JS, Weinblatt ME, Weisman MH, editors. Chapter 151. Polyarteritis nodosa and microscopic polyangiitis. Rheumatology. 2010. 5th ed. Philadelphia: Elsevier Mosby;1523–1533.3. Savige J, Davies D, Falk RJ, Jennette JC, Wiik A. Antineutrophil cytoplasmic antibodies and associated diseases: a review of the clinical and laboratory features. Kidney Int. 2000. 57:846–862.4. Uhm W. ANCA associated vasculitis. J Korean Rheum Assoc. 2010. 17:108–132.5. Jennette JC, Wilkman AS, Falk RJ. Anti-neutrophil cytoplasmic autoantibody-associated glomerulonephritis and vasculitis. Am J Pathol. 1989. 135:921–930.6. Gómez-Puerta JA, Bosch X. Anti-neutrophil cytoplasmic antibody pathogenesis in small-vessel vasculitis: an update. Am J Pathol. 2009. 175:1790–1798.7. Oh JS, Lee CK, Kim YG, Nah SS, Moon HB, Yoo B. Clinical features and outcomes of microscopic polyangiitis in Korea. J Korean Med Sci. 2009. 24:269–274.8. Jeong MJ, Kim TW, Im JY, Jeong JS, Park MR, Kim TW, et al. Microscopic polyangiitis presenting as membranoproliferative glomerulonephritis. J Korean Rheum Assoc. 2010. 17:321–325.9. Serra A, Cameron JS, Turner DR, Hartley B, Ogg CS, Neild GH, et al. Vasculitis affecting the kidney: presentation, histopathology and long-term outcome. Q J Med. 1984. 53:181–207.10. Savage CO, Winearls CG, Evans DJ, Rees AJ, Lockwood CM. Microscopic polyarteritis: presentation, pathology and prognosis. Q J Med. 1985. 56:467–483.11. Guillevin L, Durand-Gasselin B, Cevallos R, Gayraud M, Lhote F, Callard P, et al. Microscopic polyangiitis: clinical and laboratory findings in eighty-five patients. Arthritis Rheum. 1999. 42:421–430.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Microscopic Polyangiitis showing Subdural Effusion and Dural Inflammation
- A Case of Microscopic Polyangiitis
- Diagnostic Tools of Pleural Effusion
- The Utility of Pleural Adenosine Deaminase for Diagnosis of Differentiating Tuberculous Pleural Effusion in Children
- Microscopic Polyangiitis Presenting with Intracerebral Hemorrhage and Cerebral Infarction
