J Korean Soc Spine Surg.
2012 Sep;19(3):85-89. 10.4184/jkss.2012.19.3.85.
Changes in Cervical Spine Range of Motion after Laminoplasty in Cervical Spondylotic Myelopathy
- Affiliations
-
- 1Department of Orthopedic Surgery, Chungnam National University, School of Medicine, Daejeon, Korea. jsahn@cnu.ac.kr
- KMID: 1435584
- DOI: http://doi.org/10.4184/jkss.2012.19.3.85
Abstract
- STUDY DESIGN: A retrospective study.
OBJECTIVES
This study examined the cervical range of motion (ROM) of cervical spondylotic myelopathy patients, before and after open door laminoplasty. SUMMARY OF LITERATURE REVIEW: Majority of the cases regarding the change of cervical range of motion after cervical laminoplasty showed decreased range of motion, and the results were diverse.
MATERIALS AND METHODS
Of the 487 patients, who underwent open door laminoplasty at our hospital from March 1997 to March 2008, 98 had been followed for at least 2 years and had cervical flexion-extension lateral x-rays. In all patients, open door laminoplasty involved at least three segments: three, four, and five segments in 11, 52, and 35 patients, respectively. In previous cases, fixation involved sutures using suture anchors. The lordosis or kyphosis between C2 and C7 was analyzed using cervical flexion-extension lateral radiographs before and 2 years after the operation.
RESULTS
The average patient age was 62.7 (range 32-82) years; 65 patients were male and 33 were female. From preoperatively to postoperatively, the average kyphosis of cervical flexion decreased from 10.7degrees to 7.8degrees, average lordosis decreased from 21.2degrees to 14.2degrees, and cervical ROM decreased from 31.9degrees to 22.0degrees, respectively (mean 9.9degrees, 31.0%).
CONCLUSIONS
We could observe decreased cervical range of motion after cervical laminoplasty for cervical spondylotic myelopathic patients. Thus, the treatment to prevent the postoperative decrease of cervical range of motion and further study to find a new treatment are thought to be essential.
MeSH Terms
Figure
-
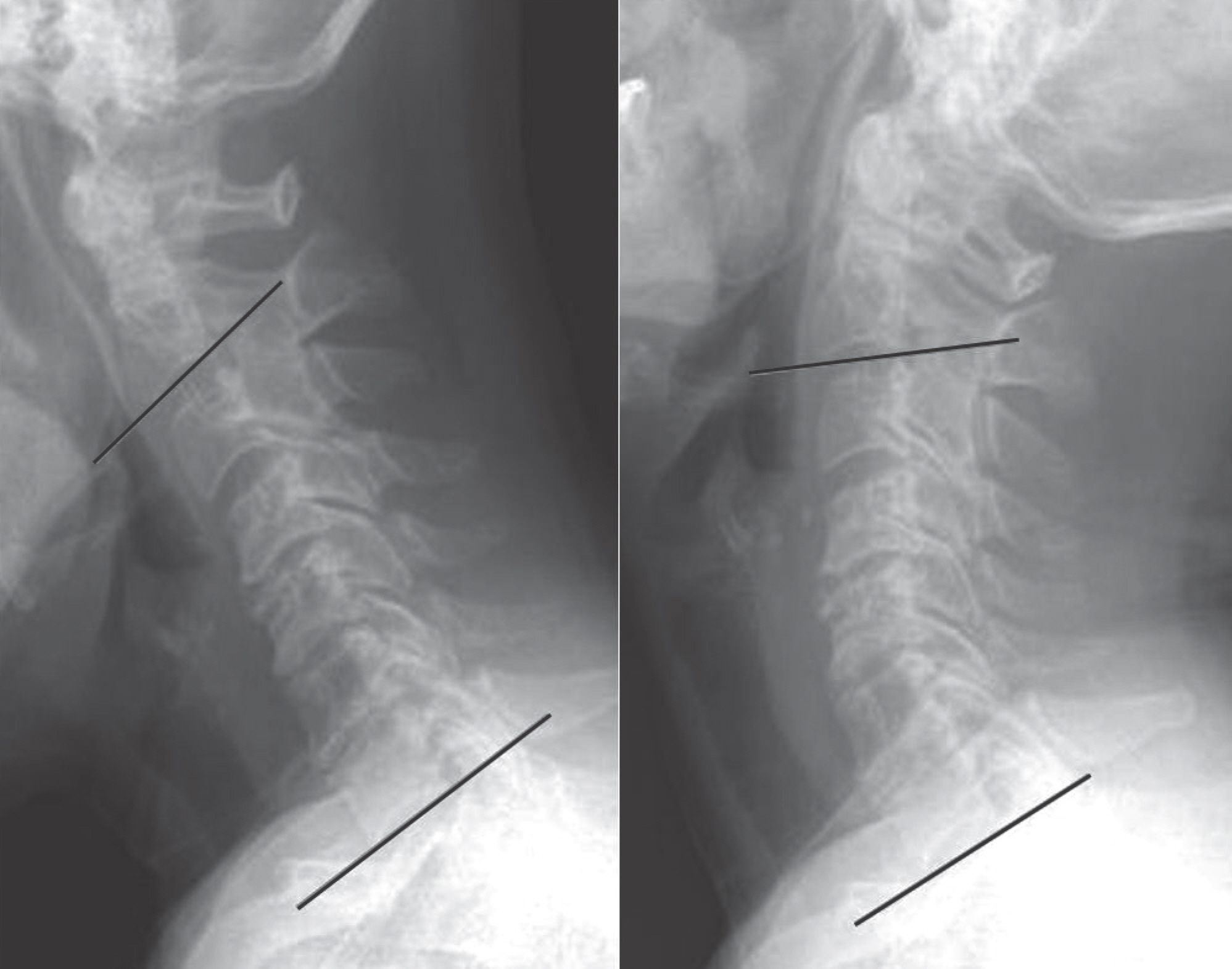
Fig 1. Flexion and extension angle of the cervical spine was measured by cobb's method from bottom of C2 to bottom of C7.
Cited by 2 articles
-
Comparison of Clinical Results according to the Complications after or during Open Door Laminoplasty Surgery for Cervical Myelopathy
Jae-Sung Ahn, June-Kyu Lee, Gi-Soo Lee, Byung-Kon Shin
J Korean Orthop Assoc. 2013;48(5):375-381. doi: 10.4055/jkoa.2013.48.5.375.Comparison between Radiological and Clinical Outcomes of Laminoplasties with Titanium Miniplates for Cervical Myelopathy
Jong-Hwa Park, Jae-Sung Ahn, Ho-Jin Lee, Byung-Kon Shin
Clin Orthop Surg. 2016;8(4):399-406. doi: 10.4055/cios.2016.8.4.399.
Reference
-
1.Herkowitz HN. A comparison of anterior cervical fusion, cervical laminectomy, and cervical laminoplasty for the surgical management of multiple level spondylotic radiculopathy. Spine (Phila Pa 1976). 1988. 13:774–80.
Article2.Herkowitz HN. The surgical treatment of cervical spondylotic radiculopathy and myelopathy. Clin Orthop Relat Res. 1989. 239:94–108.3.Kamioka Y., Yamamoto H., Tani T., Ishida K., Sawamoto T. Postoperative instability of cervical OPLL and cervical radiculomyelopathy. Spine (Phila Pa 1976). 1989. 14:1177–83.
Article4.Kawai S., Sunago K., Doi K., Saika M., Taguchi T. Cervical laminoplasty (Hattori's method). Procedure and follow-up results. Spine (Phila Pa 1976). 1988. 13:1245–50.5.Yoshida M., Otani K., Shibasaki K., Ueda S. Expansive laminoplasty with reattachment of spinous process and extensor musculature for cervical myelopathy. Spine (Phila Pa 1976). 1992. 17:491–7.
Article6.Hirabayashi K., Miyakawa J., Satomi K., Maruyama T., Wakano K. Operative results and postoperative progression of ossification among patients with ossification of cervical posterior longitudinal ligament. Spine (Phila Pa 1976). 1981. 6:354–64.
Article7.Hirabayashi K., Watanabe K., Wakano K., Suzuki N., Satomi K., Ishii Y. Expansive open-door laminoplasty for cervical spinal stenotic myelopathy. Spine (Phila Pa 1976). 1983. 8:693–9.
Article8.Hirabayashi K., Satomi K. Operative procedure and results of expansive open-door laminoplassty. Spine (Phila Pa 1976). 1988. 13:870–6.9.Hilibrand AS., Carlson GD., Palumbo MA., Jones PK., Bohl-man HH. Radyculopathy and myelopathy at segments adjacent to the site of a previous anterior cervical artrodesis. J Bone Joint Surg Am. 1999. 81:519–28.10.Vitarbo E., Sheth RN., Levi AD. Open-door expansile cervi-cal laminoplasty. Neurosurgery. 2007. 60(1 Suppl):S154–9.
Article11.Morimoto T., Ohtsuka H., Sakaki T., Kawaguchi M. Postlaminectomy cervical spinal cord compression dem-onstrated by dynamic magnetic resonance imaging. Case report. J Neurosurg. 1988. 88:155–7.12.Oiwa T., Hirabayashi K., Uzawa M., Ohira T. Experimental study on postlaminectomy deterioration of cervical spondylotic myelopathy. Influences of intradural surgery and persistent spinal block. Spine (Phila Pa 1976). 1985. 10:717–21.13.Wang MY., Green BA. Open-door cervical expansile lami-noplasty. Neurosurgery. 2004. 54:119–23.
Article14.Oyama M., Hattori S., Moriwaki N. A new method of cervical laminoplasty [in Japanese]. Cent Jpn J O rthop T rau-mat Surg. 1973. 16:792–4.15.Kaner T., Sasani M., Oktenoğ lu T., Ozer AF. Clinical out-comes following cervical laminoplasty for 19 patients with cervical spondylotic myelopathy. Turkish Neurosurgery. 2009. 19:121–6.16.Baba H., Maezawa Y., Furusawa N., Imura S., Tomita K. Flexibility and alignment of the cervical spine after laminoplasty for spondylotic myelopathy. A radiographic study. Int Orthop. 1995. 19:116–21.
Article17.Kimura I., Shingu H., Nasu Y. Long-term follow-up of cervical spondylotic myelopathy treated by canal-expansive laminoplasty. J Bone Joint Surg Br. 1995. 77:956–61.
Article18.Ogawa Y., Chiba K., Matsumoto M, et al. Long-term results after expansive open-door laminoplasty for the segmental-type of ossification of the posterior longitudinal ligament of the cervical spine: a comparison with nonseg-mental-type lesions. J Neurosurg Spine. 2005. 3:198–204.
Article19.Ratliff JK., Cooper PR. Cervical laminoplasty: a critical re-view. Neurosurg. 2003. 98:230–38.
Article20.Sakai Y., Matsuyama Y., Inoue K., Ishiguro N. Postoperative instability after lanimoplasty for cervical myelopathy with spondylolisthesis. J Spinal Disord Tech. 2005. 18:1–5.21.Vatsal DK., Husain M., Jha D., Chawla J. Square cervical laminoplasty incorporating spinous process: surgical technique. Surg Neurol. 2003. 60:131–5.
Article22.Ishibashi K. Expansive laminoplasty by sagittal splitting of the spinous process for cervical myelopathy: correlation of clinical results with morphological changes in the cervical spine. Kurume Med J. 2000. 47:135–45.
Article23.Kamioka Y., Yamamoto H., Tani T., Ishida K., Sawamoto T. Postoperative instability of cervical OPLL and cervical radiculomyelopathy. Spine (Phila Pa 1976). 1989. 14:1177–83.
Article24.Suk KS., Kim KT., Lee SH., Lim YJ., Lee KW. Changes of Range of Motion and Sagittal Alignment of the Cervical Spine after Laminoplasty. J Korean Soc Spine Surg. 2005. 12(4):247–54.
Article25.Tsuji T., Asazuma T., Masuoka K, et al. Retrospective cohort study between selective and standard C3-7 laminoplasty. Minimum 2-year follow-up study. Eur Spine J. 2007. 16:2072–7.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Change of Range of Motion at Anterior Compression of the Cervical Cord after Laminoplasty in Patients with Cervical Spondylotic Myelopathy
- Predictors of Outcome in Patients with Cervical Spondylotic Myelopathy Undergoing Unilateral Open-Door Laminoplasty
- Retraction: Sensitivity of Pyramidal Signs in Patients with Cervical Spondylotic Myelopathy
- The Factors Affecting Surgical Results in Cervical Spondylotic Myelopathy
- Effectiveness of the Laminoplasty in the Elderly Patients with Cervical Spondylotic Myelopathy
