The Factors Affecting Surgical Results in Cervical Spondylotic Myelopathy
- Affiliations
-
- 1Department of Orthopaedic Surgery, College of Medicine, Dong-A University, Busan, Korea. gylee@mail.donga.ac.kr
Abstract
- STUDY DESIGN: This is a retrospective study on the factors affecting the surgical results for cervical spondylotic myelopathy.
OBJECTIVES
We wanted to analyze the clinical and radiologic factors affecting the results of treatment for cervical spondylotic myelopathy patients who underwent anterior decompression with fusion or open door laminoplasty. SUMMARY OF THE LITERATURE REVIEW: Many authors have reported on the prognostic factors affecting the results of surgical treatment for cervical spondylotic myelopathy; some of the reported factors do affect the results, but there is a wide range of opinion about them.
MATERIALS AND METHODS
We reviewed 38 patients who underwent anterior decompression with fusion or open door laminoplasty for cervical spondylotic myelopathy between March 1999 and Dec. 2003. We analyzed the factors, including age, the duration of symptoms, the symptomatic classification, the preoperative and postoperative JOA scores, the compression ratio of the spinal cord and the surgical method. RESULT: The mean JOA score increased from 10.3+/-3.4 preoperatively to 14.9+/-4.6 postoperatively with a recovery rate of 69.0% +/- 21.24%. The preoperative JOA score and the compression ratio of the spinal cord on MRI correlated positively with the recovery rate. The patients' age showed negative correlation with the recovery rate. There is no difference between the two surgical methods for the recovery rate.
CONCLUSION
The preoperative JOA score, the patients' age and the spinal cord compression ratio on MRI are the prognostic factors affecting the surgical results, but there are no difference between the two surgical method.
Keyword
MeSH Terms
Figure
-
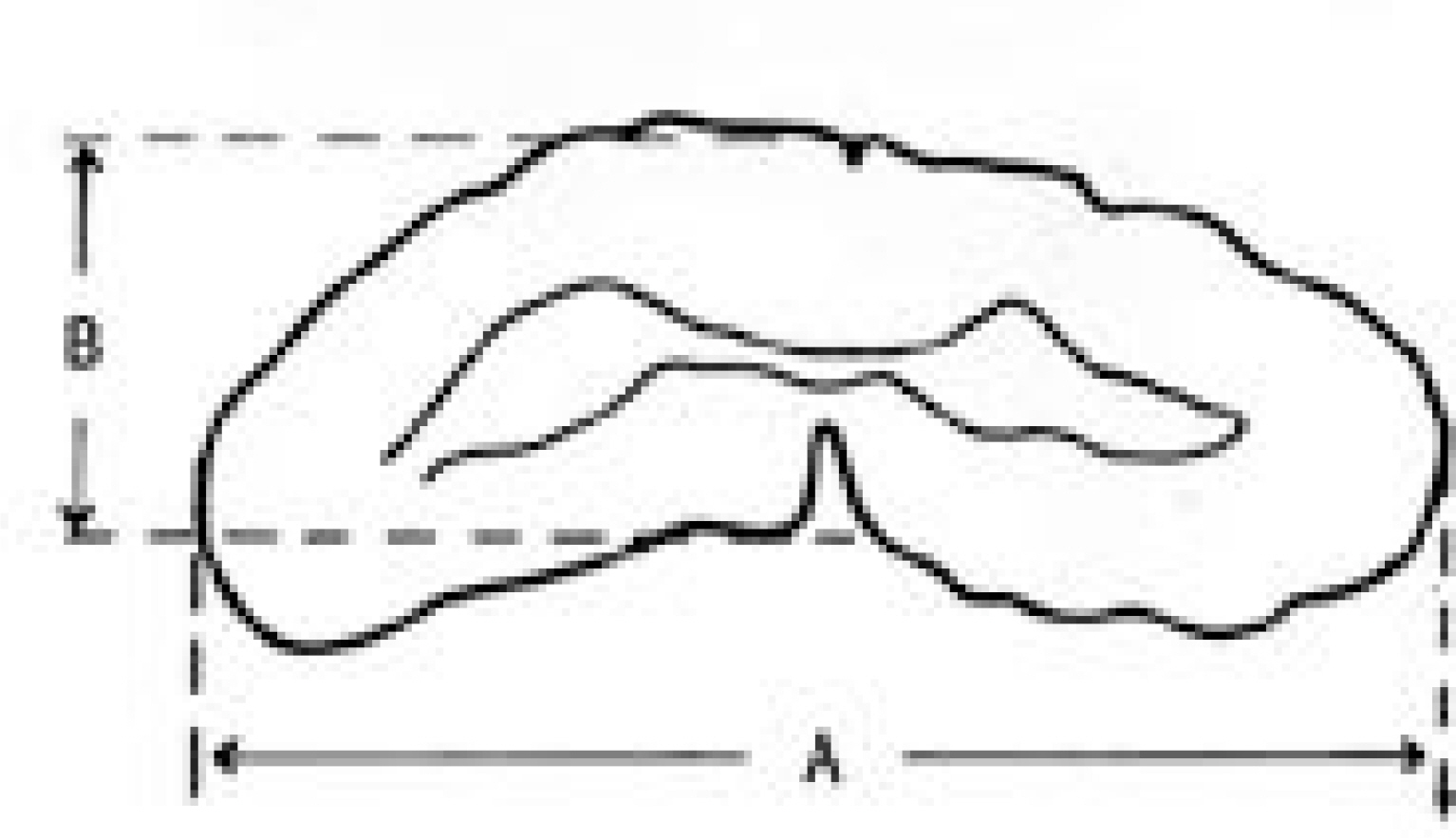
Fig. 1. Compression ratio Sagittal diameter (B) Compression ratio = Transverse diameter (A)

Fig. 2. A fifty-two years old male visited our clinic because of weakness and gait disturbance. He is classified motor system syndrome and preoperative JOA score is 10. (A) Preoperative lateral radiograph showing congenital spinal canal stenosis (Pavlov ratio: 0.67) with degenerative spondylosis. (B) T2 weighted sagittal MRI demonstrating cord compression at C3-4, C4-5 and C5-6, showing high signal change in the spinal cord at the compression site. (C) Posterative lateral radiograph showing widened of spinal canal after open door laminoplasty. (D) Posterative CT axial image shows increased canal diameter (Recovery rate : 71.43%)

Fig. 3. A forty-seven years old male visited our clinic because of upper extremity weakness and radicular pain. He is classified Brachalgia syndrome and preoperative JOA score is 12. (A) Preoperative lateral radiograph showing mild disc space narrowing at C5-6. (B) T2 weighted sagittal MRI demonstrating cord compression at C5-6. (C) Posterative lateral radiograph showing radiologic union and normal rodotic cervical curvature (Recovery rate : 80%).
Reference
-
1). Fujiwara K, Yonenobu K, Ebaras S, Yamashita K, Ono K. The prognosis of surgery for cervical compression myelopathy. An analysis of the factors involved. J Bone Joint Surg Br. 1989; 71:393–398.
Article2). Handa Y, Kubota T, Ishii H, Sato K, Tsuchida , Arai Y. Evaluation of prognostic factor and clinical outcome in eldlerly patient in whom expansive laminoplasty is performed for cervical myelopathy due to multisegmental spondylotic canal stenosis. A retrospective comparison with younger patients. J Neurosurg (spine2). 2002; 96:173–179.3). Kohono K, Kumon Y, Matsui S, Ohue S, Sasaki S. Evaluation of prognostic factors following expansive laminoplasty for cervical spinal stenotic myelopathy. Surg Neurol. 1997; 48:237–245.4). Morio Y, Teshima R, Nagashima H, Nawata K, Yamasaki D, Nanjo Y. Correlation between operative outcomes of cervical compression myelopathy and MRI of the spine cord. Spine. 2001; 26:1238–1245.5). Tanaka J, Seki N, Tokimura F, Doi K, Inoue S. Operative result of canal-expansive laminoplasty for cervical spondylotic myelopathy in eldlery patients. Spine. 1999; 24:2308–2312.6). Crandall PH, Batzdorf U. Cervical Spondylotic Myelopathy. J Neurology. 1996; 25:57–66.
Article7). Pavolov H., Torg JS, Robie B, Jahre C. Cervical spinal stenosis; determination with vertebral body ratio method. Radiology. 1987; 164:771–775.
Article8). Hirkowitz HN. A comparison of anterior cervical fusion, cervical lamininectomy, and cervical laminoplasty for the surgical management of multiple level spondylotic radiculopathy. Spine. 1988; 13:774–780.9). Simmons EH, Bhalla SK. Anterior cervical disectomy and fusion. J Bone Joint Surg. 1969; 51-B:225–237.10). Smith GW, Robinson RA. The treatment of certain cervical spine disorder by anterior removal of intervertebral disc and interbody fusion. J Bone Joint Surg Am. 1958; 40:607–624.11). Hirabayashi K, Satomi K. Operative procedure and result of expansive open door laminoplasty. Spine. 1988; 13:870–876.12). Eric T, Harry NH. Cervical spondylotic myelopathy and radiculopathy. AAOS Instructional Course Lectures. 2000; 49:339–360.13). Ono K, Ota H, Tada K, Yamamoto T. C e r v i c a l myelopathy secondary to multiple spondylotic protrusion: A clinicopathologic study. Spine. 1977; 2:109–125.14). Fujiwara K, Yonenobu K, Hiroshima K, Ebara S, Yamashita K, Ono K. Morphometry of cervical spinal cord and its relation to pathology in cases with compression myelopathy. 1988; 13:1212–1216.15). Nurick S. Natural history and the results of surgical treatment of the spinal cord disorder associated with cervical spondylosis. Brain. 1972; 95:101–105.16). Wohlert L, Buhl M, Ericken EF, et al. Treatment of cervical disc disease using Cloward's technipue. III. Evaluation of cervical spondylotic myelopathy in 138 cases. Acta Neurochir (wien). 1984; 71:121–131.17). Bailey RW, Badgley CE. Stabilization of cervical spine by anterior fusion. J Bone Joint Surg Am. 1960; 42:565–594.18). Cloward RB. The anterior approach for removal of ruptured cervical disks. J Neurology. 1958; 15:602–617.
Article19). Robinson RA, Walker AE, Ferlic DC, Wiecking DK. The result of anterior interbody fusion of the cervical spine. J Bone Joint Surg Am. 1962; 44:1569–1587.20). Han C, Won-Jong B, Jong-Wook S, Hyun B. Rationale for the combined front and back surgery in the treatment of cervical spondylotic myeloradiculopathy. J Kor Orthop Assoc. 1996; 31:33–41.21). Yonenobu K, Hosono N, Iwasaki M, Asano M, Ono K. Neurologic complications of surgery for cervical compres -sive myelopathy. Spine. 1991; 16:1277–1282.22). Tsuzuki N, Ehogshi L, Abe R, Saiki K. Paralysis of the arm after posterior decompression of the cervical spinal cord. 2. Anatomical investigation of the mechanism of paralysis. Eur spine. 1993; 2:191–196.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Prognostic Factors Affecting the Results of the Surgery for Cervical Spondylotic Myelopathy
- Anterior Cervical Decompression and Fusion for the Treatment of Cervical Spondylotic Myelopathy
- Retraction: Sensitivity of Pyramidal Signs in Patients with Cervical Spondylotic Myelopathy
- Surgical Treatment of Cervical Spondylotic Myelopathy
- Value of Surgery and Nonsurgical Approaches for Cervical Spondylotic Myelopathy: WFNS Spine Committee Recommendations
