Classification and Surgical Treatment of Symphalangism in Interphalangeal Joints of the Hand
- Affiliations
-
- 1Department of Orthopedic Surgery, Seoul National University College of Medicine, Seoul, Korea. ghbaek@snu.ac.kr
- KMID: 1245399
- DOI: http://doi.org/10.4055/cios.2012.4.1.58
Abstract
- BACKGROUND
Symphalangism is a rare congenital difference characterized by ankylosis of interphalangeal (IP) joints of the fingers and toes. In adults, there were several attempts to restore the stiff joints into mobile ones, but these treatment options resulted in poor outcomes and could not be applied to growing children. Here, we report our experiences on surgical treatment for children who had symphalangism of the hand.
METHODS
We treated 36 joints in 17 children with symphalangism of the hand using dorsal capsulotomy and collateral ligament release. The diagnoses were based on history, physical examination, and simple radiographs. Affected fingers were classified according to our grading system. Simple compressive dressing was applied using Coban after surgery. Passive range of motion (ROM) exercise was started on day one or 2 postoperative, with the help of a hand therapist and patients' parents. The patients were prescribed passive ROM exercises for at least 2 hours a day over a period of 6 months.
RESULTS
A single surgeon operated on 30 proximal IP joints, 3 distal IP joints, and 3 IP joints of the thumb. Twenty six joints were classified as grade I, and 10 as grade II. The ROM of affected joints, which was 7.8 +/- 8.1 (mean +/- SD) degrees preoperatively, increased to 46.8 +/- 18.6 degrees at final follow-up. The final ROM was significantly better in grade I joints, especially when the children had operations at ages 24 months or younger.
CONCLUSIONS
Symphalangism of the hand in children, can be restored into a mobile joint by release of the collateral ligament, a dorsal capsulotomy, and postoperative physical therapy.
Keyword
MeSH Terms
-
Age Factors
Ankylosis/radiography/surgery
Child
Child, Preschool
Female
Finger Joint/abnormalities/radiography/surgery
Humans
Infant
Joint Diseases/classification/*congenital/radiography/surgery
Ligaments/surgery
Male
Orthopedic Procedures/methods
Physical Examination
*Range of Motion, Articular
Statistics, Nonparametric
Treatment Outcome
Figure
-
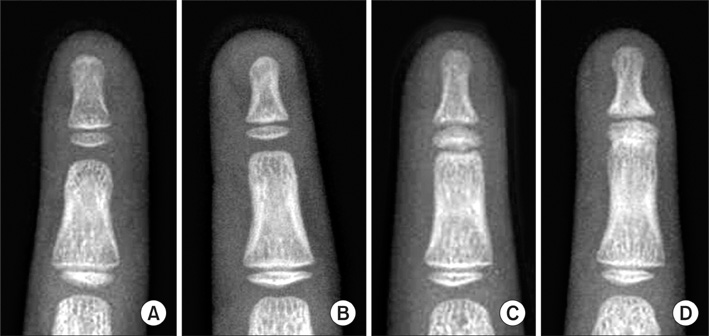
Fig. 1 Grade of symphalangism in simple radiographs. (A) Normal joint. (B) Grade I: fibrous symphalangism - mild joint space narrowing in distal interphalangeal joint. (C) Grade II: cartilaginous symphalangism - only slit of joint space is observed. (D) Grade III: bony symphalangism.

Fig. 2 Skin incision. (A) Longitudinal incision was preferred when the dorsal skin was sufficient. (B) Z-plasty incision was done when the dorsal skin of the affected joint was tight.
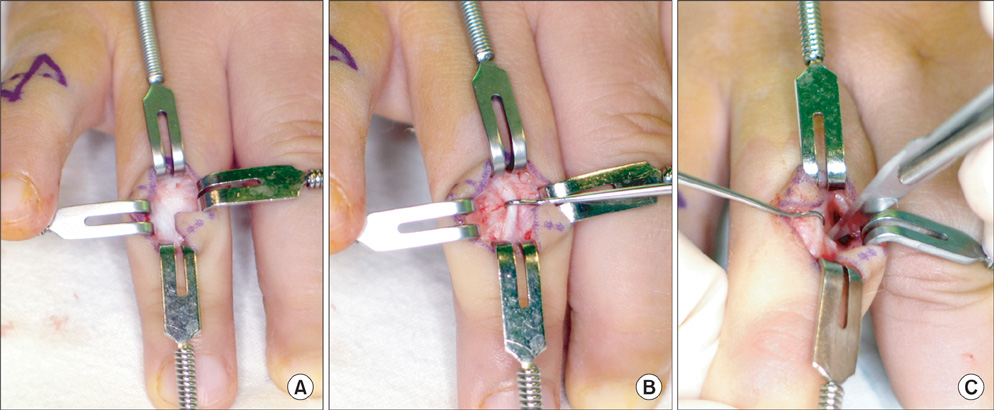
Fig. 3 Operative procedures. (A) After skin incision, extensor apparatus was exposed. (B) Extensor apparatus and joint capsule were separated from subcutaneous tissue. (C) Dorsal capsulotomy followed by release of dorsal half of both collateral ligaments were performed with a No. 11 blade, after longitudinal incision of extensor apparatus.

Fig. 4 Intraoperative passive motion before (A, C) and after (B, D) surgical release. (A, B) Full range of passive flexion were observed in 4th proximal interphalangeal (PIP) joint, and (C, D) 5th PIP joint.

Fig. 5 (A, B) There was no motion at proximal interphalangeal joint preoperatively. (C, D) The child had an operation at 17 months of age. Good range of motion was maintained at postoperative 34 months.
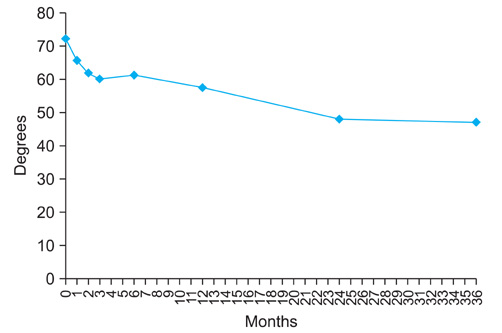
Fig. 6 Initial decrease of range of motion was significant until 2 years after the operation, however, there was no further decrease thereafter.

Fig. 7 Bony ankylosis was observed in a child who had surgery at age 7 years and 10 months.
Reference
-
1. Cushing H. Hereditary anchylosis of the proximal phalangeal joints (symphalangism). Genetics. 1916. 1(1):90–106.
Article2. Upton J. Mathes SJ, editor. Failure of differentiation and overgrowth. Plastic surgery. 2005. 2nd ed. Philadelphia: Saunders Elsevier;265–322.3. Flatt AE, Wood VE. Rigid digits or symphalangism. Hand. 1975. 7(3):197–214.
Article4. Palmieri TJ. The use of silicone rubber implant arthroplasty in treatment of true symphalangism. J Hand Surg Am. 1980. 5(3):242–244.
Article5. Dobyns J. Green DP, Hotchkiss RN, Pederson WC, editors. Symphalangism. Green's operative hand surgery. 1999. 4th ed. New York: Churchill Livingstone;470–473.6. Shibata M. Gupta A, Kay SP, Scheker LR, editors. Symphalangism. The growing hand. 2000. 1st ed. London: Mosby;289–292.7. Elkington SG, Huntsman RG. The Talbot fingers: a study in symphalangism. Br Med J. 1967. 1(5537):407–411.
Article8. Strasburger AK, Hawkins MR, Eldridge R, Hargrave RL, McKusick VA. Symphalangism: genetic and clinical aspects. Bull Johns Hopkins Hosp. 1965. 117:108–127.9. Castle JE, Bass S, Kanat IO. Hereditary symphalangism with associated tarsal synostosis and hypophalangism. J Am Podiatr Med Assoc. 1993. 83(1):1–9.
Article10. Gaal SA, Doyle JR, Larsen IJ. Symphalangism in Hawaii: a study of three distinct ethnic pedigrees. J Hand Surg Am. 1988. 13(5):783–787.
Article11. Polymeropoulos MH, Poush J, Rubenstein JR, Francomano CA. Localization of the gene (SYM1) for proximal symphalangism to human chromosome 17q21-q22. Genomics. 1995. 27(2):225–229.
Article12. Takahashi T, Takahashi I, Komatsu M, et al. Mutations of the NOG gene in individuals with proximal symphalangism and multiple synostosis syndrome. Clin Genet. 2001. 60(6):447–451.
Article13. Seemann P, Schwappacher R, Kjaer KW, et al. Activating and deactivating mutations in the receptor interaction site of GDF5 cause symphalangism or brachydactyly type A2. J Clin Invest. 2005. 115(9):2373–2381.
Article14. Upton J, Sohn SA, Glowacki J. Neocartilage derived from transplanted perichondrium: what is it? Plast Reconstr Surg. 1981. 68(2):166–174.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Double Dislocation of Interphalangeal Joints in a Single Digit: A Case Report
- Two-Phalanged Fifth Toe in Korean
- Boutonniere Deformity: A Review of Considerations before Treatment and Current Treatment Options
- Swan neck deformity: a review of its causes and treatment options
- Dislocations of the Interphalangeal Joint of the Great Tow with Interposition of a Seamoid Bone: A Report of Two Cases
