Korean J Urol.
2008 Oct;49(10):906-911. 10.4111/kju.2008.49.10.906.
Transurethral Resection of Prostate in Benign Prostatic Hyperplasia Patients with Large Prostate Volume
- Affiliations
-
- 1Department of Urology and Urological Science Institute, Yonsei University College of Medicine, Seoul, Korea. youngd74@yuhs.ac
- KMID: 1204320
- DOI: http://doi.org/10.4111/kju.2008.49.10.906
Abstract
-
PURPOSE: We investigated the safety and efficacy of transurethral resection of the prostate(TURP) in benign prostatic hyperplasia(BPH) more than 60cc by single surgeon for the relief of infravesical obstruction.
MATERIALS AND METHODS
We evaluated 211 patients treated with TURP in BPH with large prostate by single surgeon. Each group was divided by prostate volume(group 1; 60-69.9, group 2; 70-79.9, group 3; 80-89.9, group 4; 90-99.9, group 5; >100cc of prostate volume). Various parameters such as International Prostate Symptom Score(IPSS), maximal flow rate(Qmax.), postvoid residual volume(PVR), prostate volume, adenoma volume, resection time, resection prostate volume, irrigation fluid volume and complications were evaluated and compared.
RESULTS
Age of each group was not significantly different. Prostate volume, adenoma volume, resection time, Resection volume, irrigation volume of each groups were different significantly. But, resection volume/resection time and irrigation volume/resection time were not different significantly. Mean resection volume/resection time was 1.34g/min, and mean irrigation volume/resection time was 315.8ml/min. And intraoperative and postoperative complications of each group were not different. Mean postoperative change of Hb was 2.0+/-1.1g/dl. Postoperative parameters(IPSS, Qmax, PVR) were improved significantly. Only 2 patients needed transfusion in group 5. No urinary incontinence and TUR syndrome in each group was observed.
CONCLUSIONS
TURP by experienced surgeon is a safe and effective treatment in BPH patients with large prostates for relief of infravesical obstruction.
MeSH Terms
Figure
-
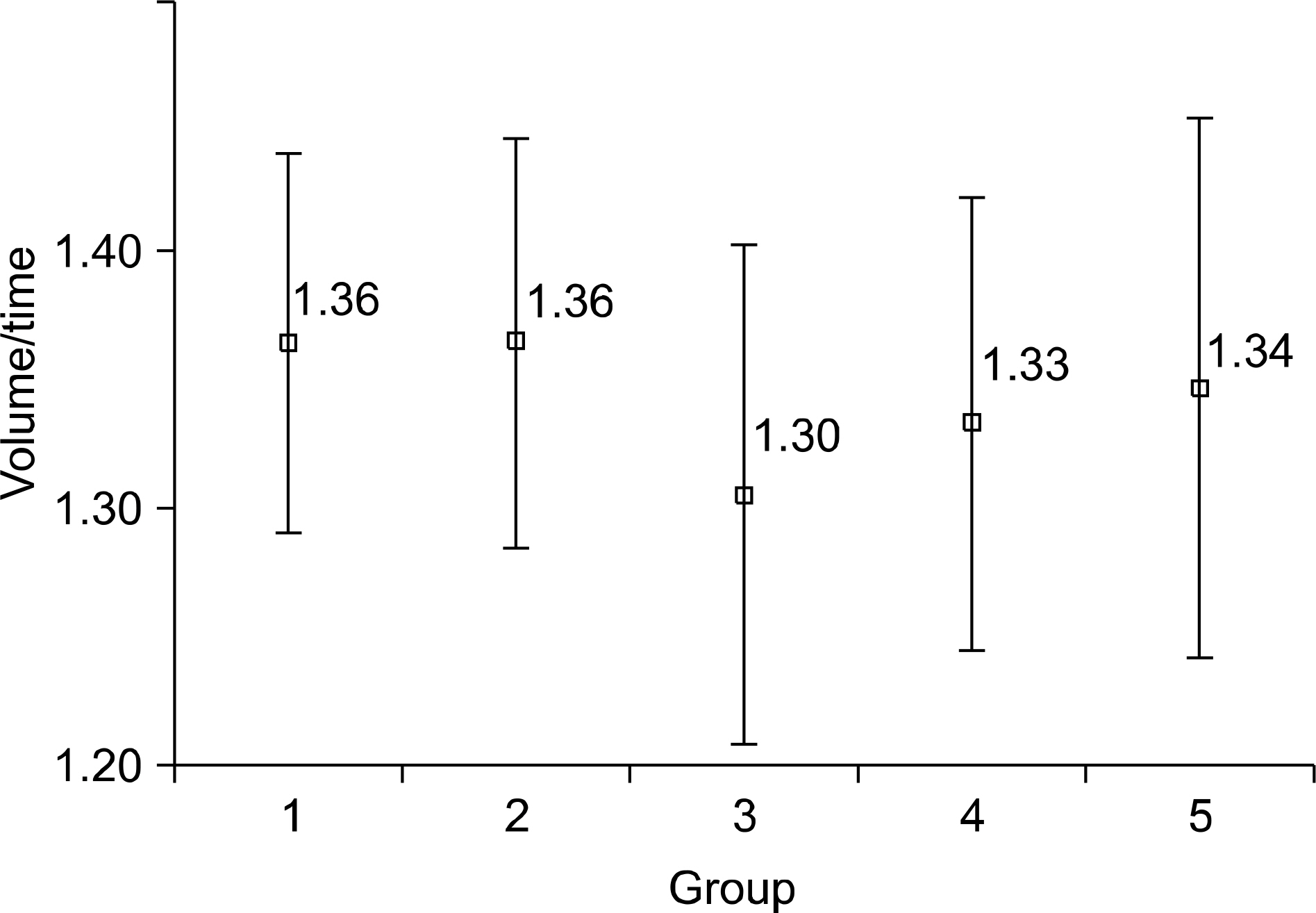
Fig. 1. Resection volume/resection time (g/min) in each group.
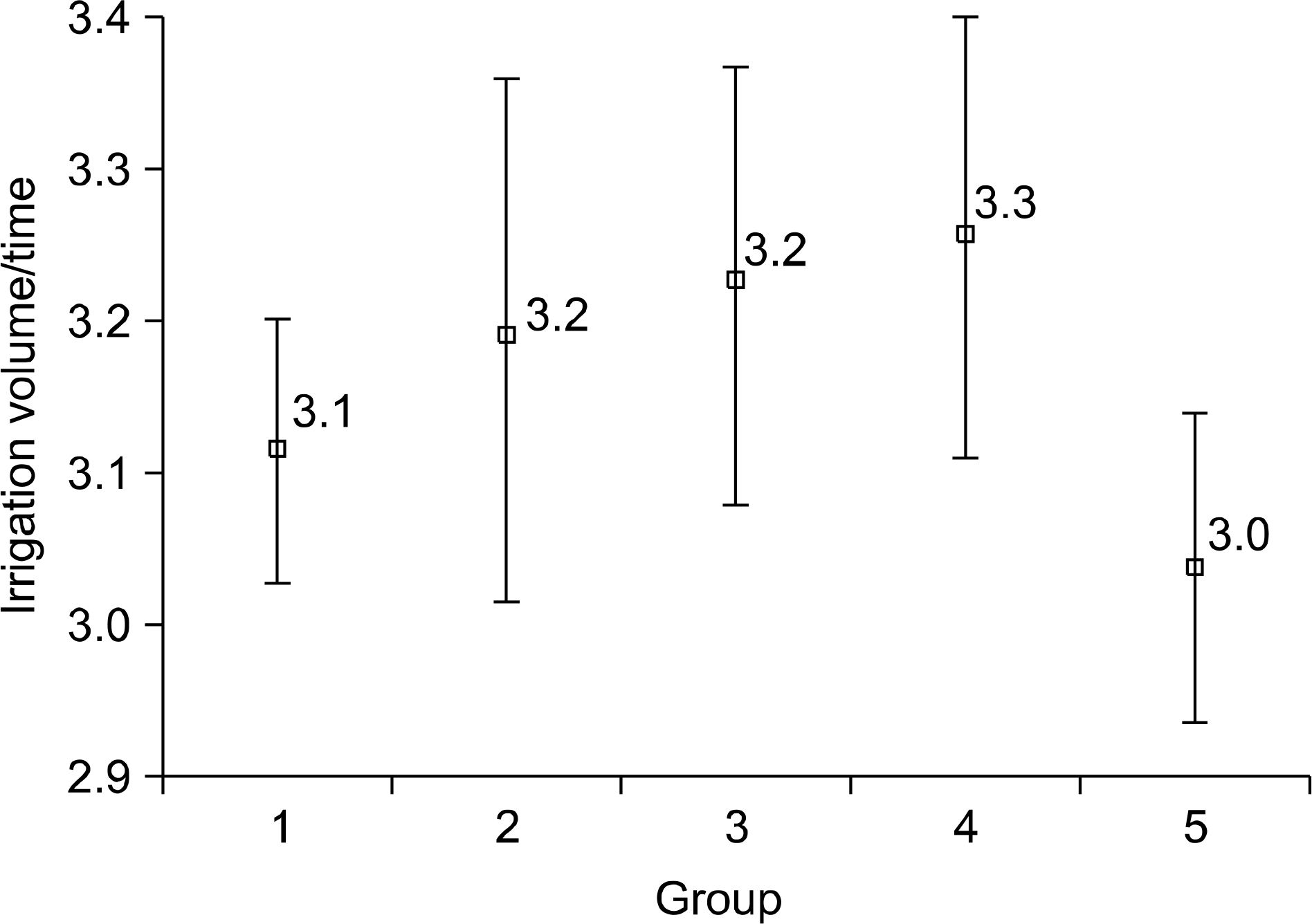
Fig. 2. Irrigation volume/resection time (100ml/min) in each group.
Reference
-
References
1. Barba M, Leyh H, Hartung R. New technologies in transurethral resection of the prostate. Curr Opin Urol. 2000; 10:9–14.
Article2. Montorsi F, Guazzoni G, Bergamaschi F, Consonni P, Matozzo V, Barbieri L, et al. Long-term clinical reliability of transurethral and open prostatectomy for benign prostatic obstruction: a term of comparison for nonsurgical procedures. Eur Urol. 1993; 23:262–6.3. Tubaro A, Carter S, Hind A, Vicentini C, Miano L. A prospective study of the safety and efficacy of suprapubic transvesical prostatectomy in patients with benign prostatic hyperplasia. J Urol. 2001; 166:172–6.
Article4. Hakenberg OW, Helke C, Manseck A, Wirth MP. Is there a relationship between the amount of tissue removed at transurethral resection of the prostate and clinical improvement in benign prostatic hyperplasia. Eur Urol. 2001; 39:412–7.
Article5. Nouira Y, Kbaier I, Attyaoui F, Horchani A. How did the endoscopic video camera change our practice in transurethral resection of the prostate? A retrospective study of 200 cases. J Endourol. 2002; 16:763–5.
Article6. Rassweiler J, Teber D, Kuntz R, Hofmann R. Complications of transurethral resection of the prostate (TURP)–incidence, management, and prevention. Eur Urol. 2006; 50:969–79.
Article7. Muzzonigro G, Milanese G, Minardi D, Yehia M, Galosi AB, Dellabella M. Safety and efficacy of transurethral resection of prostate glands up to 150ml: a prospective comparative study with 1 year of followup. J Urol. 2004; 172:611–5.8. Cho JS, Kim CI, Seong DH, Kim HS, Kim YS, Kim SJ, et al. Cut-off point of large prostate volume for the patients with benign prostatic hyperplasia. Korean J Urol. 2005; 46:1246–50.9. Madersbacher S, Marberger M. Is transurethral resection of the prostate still justified? BJU Int. 1999; 83:227–37.
Article10. AUA Practice Guidelines Committee. AUA guideline on management of benign prostatic hyperplasia (2003). Chapter 1: Diagnosis and treatment recommendations. J Urol. 2003; 170:530–47.11. Roehrborn CG, Bartsch G, Kirby R, Andriole G, Boyle P, de la Rosette J, et al. Guidelines for the diagnosis and treatment of benign prostatic hyperplasia: a comparative, international overview. Urology. 2001; 58:642–50.
Article12. Han M, Partin AW. Retropubic and suprapubic open prostatectomy. Wein AJ, Novick AC, Partin AW, Perters CA, editors. editors.Campbell-Walsh urology. 9th ed.Philadelphia: Saunders;2007. p. 2845–53.
Article13. Mebust WK, Holtgrewe HL, Cockett AT, Peters PC. Transurethral prostatectomy: immediate and postoperative complications. A cooperative study of 13 participating institutions evaluating 3,885 patients. J Urol. 1989; 141:243–7.14. Olsson J, Nilsson A, Hahn RG. Symptoms of the transurethral resection syndrome using glycine as the irrigant. J Urol. 1995; 154:123–8.
Article15. Serretta V, Morgia G, Fondacaro L, Curto G, Lo bianco A, Pirritano D, et al. Open prostatectomy for benign prostatic enlargement in southern Europe in the late 1990s: a contemporary series of 1,800 interventions. Urology. 2002; 60:623–7.
Article16. Moody JA, Lingeman JE. Holmium laser enucleation for prostate adenoma greater than 100 gm: comparison to open prostatectomy. J Urol. 2001; 165:459–62.17. Kuntz RM, Lehrich K. Transurethral holmium laser enucleation versus transvesical open enucleation for prostate adenoma greater than 100 gm: a randomized prospective trial of 120 patients. J Urol. 2002; 168:1465–9.
Article18. Kuo RL, Kim SC, Lingeman JE, Paterson RF, Watkins SL, Simmons GR, et al. Holmium laser enucleation of prostate (HoLEP): the methodist hospital experience with greater than 75 gram enucleations. J Urol. 2003; 170:149–52.
Article19. Sandhu JS, Casey NG, Vanderbrink BA, Egan C, Kaplan SA, Alexis E. High power potassium titanly phosphate laser vaporization of the prostate for treatment of benign prostatic hyperplasia in men with large prostates. Urology. 2004; 64:1155–9.20. Tasci AI, Tugcu V, Sahin S, Zorluoglu F. Rapid communication: photoselective vaporization of the prostate versus transurethral resection of the prostate for the large prostate: A prospective nonrandomized bicenter trial with 2-year followup. J Endourol. 2008; 22:347–53.
Article21. Yoon JH, Chung JI, Choi SH. The effect of a transition zone resection rate of the transurethral resection of prostate (TURP) according to the prostate volume. Korean J Urol. 2005; 46:49–56.22. Liu CK, Lee WK, Ko MC, Chiang HS, Wan KS. Transurethral electrovapor resection versus standard transurethral resection treatment for a large prostate: a 2-year follow-up study conducted in Taiwan. Urol Int. 2006; 76:144–9.
Article23. Gupta NP, Singh A, Kumar R. Transurethral vapor resection of prostate is a good alternative for prostates >70g. J Endourol. 2007; 21:1543–6.24. Matthews GJ, Motta J, Fracehia JA. The accuracy of transrectal ultrasound prostate volume estimation: clinical correlations. J Clin Ultrasound. 1996; 24:501–5.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Efficacy of Transurethral Resection of Prostate in the Patients with Benign Prostatic Hyperplasia of 30gm or Less
- Comparison of the Finding of Transrectal Ultrasonography and the Result of Transurethral Resection of Prostate according to the Histologic Types in Benign Prostatic Hyperplasia
- Clinical Observation on Transurethral Resection of Prostate and Suprapubic Prostatectomy for Benign Prostatic Hypertrophy
- Long-Term Results of Transurethral Resection of the Prostate for Large Benign Prostatic Hyperplasia: A Comparative Study with Open Prostatectomy
- Fluid extravasation caused by bladder perforation during bipolar transurethral resection using saline solution: a case report
