FDG PET/CT and Mediastinal Nodal Metastasis Detection in Stage T1 Non-Small Cell Lung Cancer: Prognostic Implications
- Affiliations
-
- 1Department of Radiology and Center for Imaging Science, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea. kyungs.lee@samsung.com
- 2Department of Thoracic Surgery, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
- 3Department of Nuclear Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
- 4Division of Pulmonary and Critical Care Medicine, Department of Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
- 5Division of Medical Oncology, Department of Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
- KMID: 1118868
- DOI: http://doi.org/10.3348/kjr.2008.9.6.481
Abstract
OBJECTIVE
We aimed to compare the prognoses of patients with pathologically true negative (P-TN) N2 and PET/CT false negative (FN) results in stage T1 non-small cell lung cancer (NSCLC). MATERIALS AND METHODS: Our institutional review board approved this retrospective study with a waiver of informed consent. The study included 184 patients (124 men and 60 women; mean age, 59 years) with stage T1 NSCLC who underwent an integrated PET/CT and surgery. After estimating the efficacy of PET/CT for detecting N2 disease, we determined and compared disease-free survival (DFS) rates in three groups (P-TN [n = 161], PET/CT FN [n = 12], and PET/CT true positive [TP, n = 11]) using the Kaplan-Meier analysis and log-rank test. RESULTS: Pathologic N2 disease was observed in 23 (12%) patients. PET/CT had an N2 disease detection sensitivity of 48% (11 of 23 patients), a specificity of 95% (153 of 161), and an accuracy of 89% (164 of 184). The 3-year DFS rate in the PET/CT FN group (31%, 95% confidence interval [CI]; 13.6-48.0%) was similar to that of the TP group (16%, 95% CI; 1.7-29.5%) (p = 0.649), but both groups had significantly shorter DFS rates than the P-TN group (77%, 95% CI; 72.0-81.2%) (p < 0.001). CONCLUSION: The PET/CT shows a high specificity, but low sensitivity for detecting N2 disease in stage T1 NSCLC. Patients with PET/CT FN N2 disease have survival rates similar to PET/CT TP N2 disease patients, which are both substantially shorter than the survival rate of P-TN patients.
MeSH Terms
-
Adult
Aged
Aged, 80 and over
Carcinoma, Non-Small-Cell Lung/mortality/*radiography/*radionuclide imaging
Disease-Free Survival
Female
Fluorodeoxyglucose F18/diagnostic use
Humans
Lung Neoplasms/mortality/*radiography/*radionuclide imaging
Lymphatic Metastasis
Male
Mediastinum
Middle Aged
*Positron-Emission Tomography
Prognosis
Radiopharmaceuticals/diagnostic use
Sensitivity and Specificity
Survival Rate
*Tomography, X-Ray Computed
Figure
-
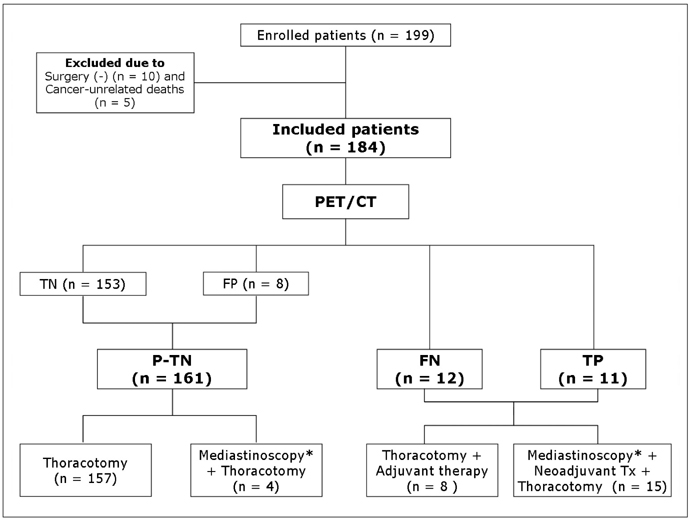
Fig. 1 Flowchart illustrating study design and number of patients enrolled in this study from each group. P-TN = pathologically true negative, TN = true negative, FP = false positive, FN = false negative, TP = true positive, *Neither FDG uptake amount of primary tumor or PET/CT mediastinal nodal FDG uptake result was determinant for performing mediastinoscopy.

Fig. 2 False negative PET/CT interpretation for mediastinal nodal staging in 42-year-old woman with stage T1 adenocarcinoma of lung showing recurrent disease on follow-up examination. A, B. Transverse (A) and coronal (B) images of initial PET/CT show 20-mm-sized nodule (arrows) in right lower lobe (maximum SUV = 9.5). There was no identifiable mediastinal uptake, but thoracotomy disclosed malignant cells in right lower paratracheal (nodal station 4R) and subcarinal (station 7) nodes. C, D. 9-month follow-up transverse CT (C) and coronal PET (D) scans demonstrate 20-mm-sized right anterior diaphragmatic node (arrows) with high amount FDG uptake (maximum SUV = 7.0), which is suggestive of recurrent disease.
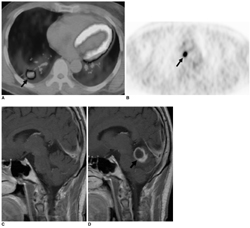
Fig. 3 True positive PET/CT interpretation for mediastinal nodal staging in 46-year-old man with stage T1 adenocarcinoma of lung showing metastatic disease on follow-up examination. A, B. Transverse images of initial PET/CT show 29-mm-sized nodule (arrow in A) with high amount of FDG uptake (maximum SUV = 10.4) in right lower lobe and right lower paratracheal lymph node (nodal station 4R, arrow in B) of high FDG uptake. Nodes contained malignant cells upon examination of mediastinoscopic biopsy. C, D. Initial (C) and follow-up (D) enhanced sagittal T1-weighted MR images over seven month follow-up period show newly developed metastatic nodule (arrow in D) in cerebellar vermis.

Fig. 4 Diagram illustrating comparison of overall survival of 184 patients belonging to pathologic true negative (TN), PET/CT false negative (FN), and true positive (TP) groups. Survival is significantly better in true negative group than false negative or true positive group.
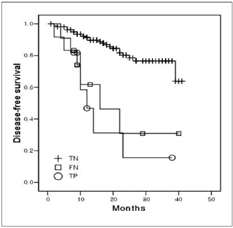
Fig. 5 Diagram illustrating comparison of disease-free survival of 184 patients belonging to pathologic true negative (TN), PET/CT false negative (FN), and true positive (TP) groups. Disease-free survival is significantly greater in true negative group than false negative or true positive group.
Reference
-
1. Shim SS, Lee KS, Kim BT, Chung MJ, Lee EJ, Han J, et al. Non-small cell lung cancer: prospective comparison of integrated FDG PET/CT and CT alone for preoperative staging. Radiology. 2005. 236:1011–1019.2. Kim BT, Lee KS, Shim SS, Choi JY, Kwon OJ, Kim H, et al. Stage T1 non-small cell lung cancer: preoperative mediastinal nodal staging with integrated FDG PET/CT - a prospective study. Radiology. 2006. 241:501–509.3. Kim YK, Lee KS, Kim BT, Choi JY, Kim H, Kwon OJ, et al. Mediastinal nodal staging of nonsmall cell lung cancer using integrated 18F-FDG PET/CT in a tuberculosis-endemic country: diagnostic efficacy in 674 patients. Cancer. 2007. 109:1068–1077.4. Pearson FG, DeLarue NC, Ilves R, Todd TR, Cooper JD. Significance of positive superior mediastinal nodes identified at mediastinoscopy in patients with resectable cancer of the lung. J Thorac Cardiovasc Surg. 1982. 83:1–11.5. Mountain CF, Dresler CM. Regional lymph node classification for lung cancer staging. Chest. 1997. 111:1718–1723.6. Ahuja V, Coleman RE, Herndon J, Patz EF Jr. The prognostic significance of fluorodeoxyglucose positron emission tomography imaging for patients with nonsmall cell lung carcinoma. Cancer. 1998. 83:918–924.7. Sasaki R, Komaki R, Macapinlac H, Erasmus J, Allen P, Forster K, et al. [18F]fluorodeoxyglucose uptake by positron emission tomography predicts outcome of non-small-cell lung cancer. J Clin Oncol. 2005. 23:1136–1143.8. Downey RJ, Akhurst T, Gonen M, Vincent A, Bains MS, Larson S, et al. Preoperative F-18 fluorodeoxyglucose-positron emission tomography maximal standardized uptake value predicts survival after lung cancer resection. J Clin Oncol. 2004. 22:3255–3260.9. Higashi K, Ueda Y, Arisaka Y, Sakuma T, Nambu Y, Oguchi M, et al. 18F-FDG uptake as a biologic prognostic factor for recurrence in patients with surgically resected non-small cell lung cancer. J Nucl Med. 2002. 43:39–45.10. Cerfolio RJ, Bryant AS, Ohja B, Bartolucci AA. The maximum standardized uptake values on positron emission tomography of a non-small cell lung cancer predict stage, recurrence, and survival. J Thorac Cardiovasc Surg. 2005. 130:151–159.11. Ohtsuka T, Nomori H, Watanabe K, Kaji M, Naruke T, Suemasu K, et al. Prognostic significance of [(18)F]fluorodeoxyglucose uptake on positron emission tomography in patients with pathologic stage I lung adenocarcinoma. Cancer. 2006. 107:2468–2473.12. van Baardwijk A, Dooms C, van Suylen RJ, Verbeken E, Hochstenbag M, Dehing-Oberije C, et al. The maximum uptake of (18)F-deoxyglucose on positron emission tomography scan correlates with survival, hypoxia inducible factor-1alpha and GLUT-1 in non-small cell lung cancer. Eur J Cancer. 2007. 43:1392–1398.13. Vansteenkiste JF, Stroobants SG, Dupont PJ, De Leyn PR, Verbeken EK, Deneffe GJ, et al. Prognostic importance of the standardized uptake value on (18)F-fluoro-2-deoxy-glucose-positron emission tomography scan in non-small-cell lung cancer: an analysis of 125 cases. Leuven Lung Cancer Group. J Clin Oncol. 1999. 17:3201–3206.14. Nomori H, Watanabe K, Ohtsuka T, Naruke T, Suemasu K, Kobayashi T, et al. Fluorine 18-tagged fluorodeoxyglucose positron emission tomographic scanning to predict lymph node metastasis, invasiveness, or both, in clinical T1 N0 M0 lung adenocarcinoma. J Thorac Cardiovasc Surg. 2004. 128:396–401.15. Nomori H, Watanabe K, Ohtsuka T, Naruke T, Suemasu K, Uno K. Evaluation of F-18 fluorodeoxyglucose (FDG) PET scanning for pulmonary nodules less than 3 cm in diameter, with special reference to the CT images. Lung Cancer. 2004. 45:19–27.16. Sagawa M, Higashi K, Sugita M, Ueda Y, Maeda S, Toga H, et al. Fluorodeoxyglucose uptake correlates with the growth pattern of small peripheral pulmonary adenocarcinoma. Surg Today. 2006. 36:230–234.17. Vesselle H, Freeman JD, Wiens L, Stern J, Nguyen HQ, Hawes SE, et al. Fluorodeoxyglucose uptake of primary non-small cell lung cancer at positron emission tomography: new contrary data on prognostic role. Clin Cancer Res. 2007. 13:3255–3263.18. Vesselle H, Turcotte E, Wiens L, Schmidt R, Takasugi JE, Lalani T, et al. Relationship between non-small cell lung cancer fluorodeoxyglucose uptake at positron emission tomography and surgical stage with relevance to patient prognosis. Clin Cancer Res. 2004. 10:4709–4716.19. Vesselle H, Schmidt RA, Pugsley JM, Li M, Kohlmyer SG, Vallires E, et al. Lung cancer proliferation correlates with [F-18]fluorodeoxyglucose uptake by positron emission tomography. Clin Cancer Res. 2000. 6:3837–3844.20. Flieder DB, Port JL, Korst RJ, Christos PJ, Levin MA, Becker DE, et al. Tumor size is a determinant of stage distribution in t1 non-small cell lung cancer. Chest. 2005. 128:2304–2308.21. Port JL, Kent MS, Korst RJ, Libby D, Pasmantier M, Altorki NK. Tumor size predicts survival within stage IA non-small cell lung cancer. Chest. 2003. 124:1828–1833.22. Warren WH, Faber LP. Segmentectomy versus lobectomy in patients with stage I pulmonary carcinoma. Five-year survival and patterns of intrathoracic recurrence. J Thorac Cardiovasc Surg. 1994. 107:1087–1093.23. Okada M, Nishio W, Sakamoto T, Uchino K, Yuki T, Nakagawa A, et al. Effect of tumor size on prognosis in patients with non-small cell lung cancer: the role of segmentectomy as a type of lesser resection. J Thorac Cardiovasc Surg. 2005. 129:87–93.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Role of PET in Staging Non-Small Cell Lung Cancer
- Accuracy of Nodal Staging with Integrated PET/CT Scanning in Non-small Cell Lung Cancer
- Significant Mismatch between FDG Uptake and Size after Chemotherapy in a Patient with Non-small Cell Lung Cancer
- Thoracic nodal staging in non-small cell lung cancer by FDG-PET
- The Ability of FDG Uptake Ratio and Glut-1 Expression to Predict Mediastinal Lymph Node Metastasis in Resected Non-small Cell Lung Cancer
