Ankle Deformity Secondary to Acquired Fibular Segmental Defect in Children
- Affiliations
-
- 1Department of Orthopaedic Surgery, St. Mary's Hospital, The Catholic University of Korea School of Medicine, Seoul, Korea. skrhee@catholic.ac.kr
- KMID: 999438
- DOI: http://doi.org/10.4055/cios.2010.2.3.179
Abstract
- BACKGROUND
The authors report the long-term effect of acquired pseudoarthrosis of the fibula on ankle development in children during skeletal growth, and the results of a long-term follow-up of Langenskiold's supramalleolar synostosis to correct an ankle deformity induced by an acquired fibular segmental defect in children.
METHODS
Since 1980, 19 children with acquired pseudoarthrosis of the fibula were treated and followed up for an average of 11 years. Pseudoarthrosis was the result of a fibulectomy for tumor surgery, osteomyelitis of the fibula and traumatic segmental loss of the fibula in 10, 6, and 3 cases, respectively. Initially, a Langenskiold's operation (in 4 cases) and fusion of the lateral malleolus to the distal tibial epiphysis (in 1 case) were performed, whereas only skeletal growth was monitored in the other 14 cases. After a mean follow-up of 11 years, the valgus deformity and external tibial torsion of the ankle joint associated with proximal migration of the lateral malleolus needed to be treated with a supramallolar osteotomy in 12 cases (63%). These ankle deformities were evaluated using the serial radiographs and limb length scintigraphs.
RESULTS
In all cases, early closure of the lateral part of the distal tibial physis, upward migration of the lateral malleolus, unstable valgus deformity and external tibial torsion of the ankle joint developed during a mean follow-up of 11 years (range, 5 to 21 years). The mean valgus deformity and external tibial torsion of the ankle at the final follow-up were 15.2degrees (range, 5degrees to 35degrees) and 10degrees (range, 5degrees to 12degrees), respectively. In 12 cases (12/19, 63%), a supramalleolar corrective osteotomy was performed but three children had a recurrence requiring an additional supramalleolar corrective osteotomy 2-4 times.
CONCLUSIONS
A valgus deformity and external tibial torsion are inevitable after acquired pseudoarthrosis of the fibula in children. Both Langenskiold supramalleolar synostosis to prevent these ankle deformities and supramalleolar corrective osteotomy to correct them in children are effective initially. However, both procedures cannot maintain the permanent ankle stability during skeletal maturity. Therefore any type of prophylactic surgery should be carried out before epiphyseal closure of the distal tibia occurs, but the possibility of a recurrence of the ankle deformities and the need for final corrective surgery after skeletal maturity should be considered.
Keyword
MeSH Terms
Figure
-
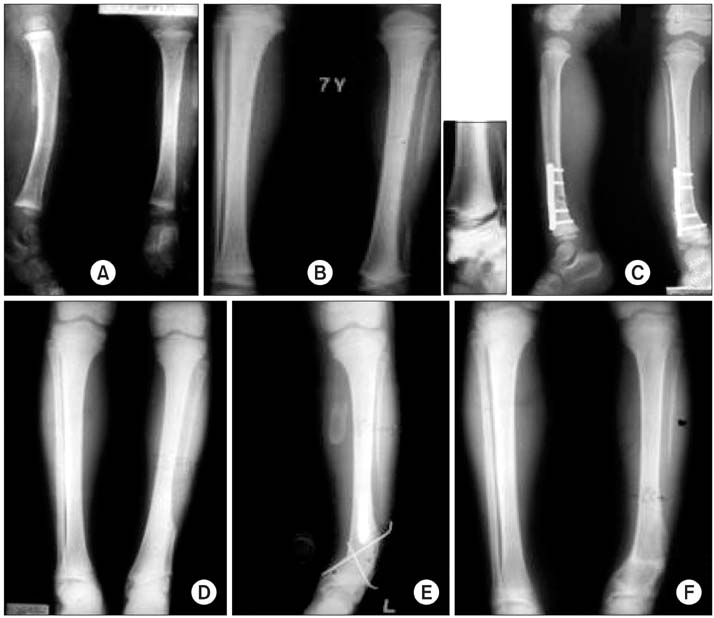
Fig. 1 (A) Radiographs of the lower leg at 3 years of age show a large segmental fibular defect by chronic osteomyelitis. (B, C) Four years later, serial radiographs show a valgus deformity of the ankle due to upward migration of the distal fibula and partial epiphyseal closure of the lateral part of the distal tibia, and a supramalleolar corrective osteotomy and Langenskiold's distal tibio-fibular synostosis was performed to correct the deformity. (D) At age 18, 11 years after the Langenskiold's operation, the radiographs show solid fusion between the distal tibia and fibula, but the valgus deformity had progressed by 23° and his leg was shortened by 1.2 cm. (E) Second supramalleolar corrective osteotomy: 8° of varus ankle position is shown to prevent the recurrence of the valgus deformity during skeletal growth. (F) At age 24, 6 years after the second supramalleolar osteotomy, the joint line between the ankle and knee was relatively parallel but the limb length discrepancy remained.

Fig. 2 (A) Radiographs of the lower leg of a 2-year-old female show a large segmental fibular loss and the small remaining lateral malleolar epiphysis by chronic osteomyelitis. (B) One year later at age 3, radiographs show a mild valgus deformity (15°) of the ankle, but there is a relatively good ankle shape with stability. (C) Fourteen years later at age 16, the valgus ankle deformity was increased to 25°. (D) Radiographs of the supramalleolar corrective osteotomy.

Fig. 3 (A) A 3-year-old female was treated with a segmental fibulectomy by the multiloculated osteofibrous dysplasia on the tibia and fibula. Four years later, the radiographs show pseudoarthrosis of the fibula with anterior tibial bowing and upward migration of the lateral malleolus. (B) Two years later at age 9, the radiographs show gradual upward migration of the distal fibula and early closure of the lateral part of the distal tibial epiphysis, resulting in a valgus ankle deformity. (C) Two years later at age 11, valgus and external tibial torsion is progressing. (D) One year later at age 12, the last follow-up radiographs show more increased valgus ankle deformity of 25° and almost closed thelateral physis of the distal tibia.

Fig. 4 Proposed mechanism for gradual development of the valgus ankle deformity due to acquired fibular pseudoarthrosis in growing children. In a normal ankle, even axial loading was applied to the physis of the distal tibia and fibula, and harmonious growth occurred. On the other hand, in pseudoarthrosis, the valgus deformity increased due to the loss of a normal physiological load (pressure) from the proximal fibula to the distal physis, and the upward dragging of the remaining distal fibula by the inelastic contracted soft tissue scar around the pseudoarthrosis (tethering effect), and asymmetrical suppression of epiphyseal growth. P: Pressure.
Reference
-
1. Wiltse LL. Valgus deformity of the ankle: a sequel to acquired or congenital abnormalities of the fibula. J Bone Joint Surg Am. 1972. 54(3):595–606.2. Paluska DJ, Blount WP. Ankle valgus after the Grice subtalar stabilization: the late evaluation of a personal series with a modified technic. Clin Orthop Relat Res. 1968. (59):137–146.3. Hsu LC, Yau AC, O'Brien JP, Hodgson AR. Valgus deformity of the ankle resulting from fibular resection for a graft in subtalar fusion in children. J Bone Joint Surg Am. 1972. 54(3):585–594.
Article4. Hsu LC, O'Brien JP, Yau AC, Hodgson AR. Valgus deformity of the ankle in children with fibular pseudarthrosis: results of treatment by bone-grafting of the fibula. J Bone Joint Surg Am. 1974. 56(3):503–510.5. Moon MS, Rhee SK, Lee HD, Ju IT, Nam SH. Valgus ankle secondary to acquired fibular pseudoarthrosis in children. Long-term results of the Langenskiold operation. Bull Hosp Jt Dis. 1997. 56(3):149–153.6. Langenskiold A. Pseudarthrosis of the fibula and progressive valgus deformity of the ankle in children: treatment by fusion of the distal tibial and fibular metaphyses: review of three cases. J Bone Joint Surg Am. 1967. 49(3):463–470.7. Lambert KL. The weight-bearing function of the fibula: a strain gauge study. J Bone Joint Surg Am. 1971. 53(3):507–513.8. Basmajian JV, Slonecker CE. Grant's method of anatomy. 1972. 8th ed. Baltimore: Williams & Wilkins.9. Gonzalez-Herranz P, del Rio A, Burgos J, Lopez-Mondejar JA, Rapariz JM. Valgus deformity after fibular resection in children. J Pediatr Orthop. 2003. 23(1):55–59.
Article10. Dias LS. Valgus deformity of the ankle joint: pathogenesis of fibular shortening. J Pediatr Orthop. 1985. 5(2):176–180.11. Burkus JK, Moore DW, Raycroft JF. Valgus deformity of the ankle in myelodysplastic patients: correction by stapling of the medial part of the distal tibial physis. J Bone Joint Surg Am. 1983. 65(8):1157–1162.
Article12. Arkin AM, Katz JF. The effects of pressure on epiphyseal growth; the mechanism of plasticity of growing bone. J Bone Joint Surg Am. 1956. 38(5):1056–1076.13. Strobino LJ, French GO, Colonna PC. The effect of increasing tensions on the growth of epiphyseal bone. Surg Gynecol Obstet. 1952. 95(6):694–700.14. Yang KY, Lee EH. Isolated congenital pseudoarthrosis of the fibula. J Pediatr Orthop B. 2002. 11(4):298–301.
Article15. Cho TJ, Choi IH, Chung CY, Yoo WJ, Lee SH, Suh SW. Isolated congenital pseudarthrosis of the fibula: clinical course and optimal treatment. J Pediatr Orthop. 2006. 26(4):449–454.16. Beals RK, Shea M. Correlation of chronological age and bone age with the correction of ankle valgus by surface epiphysiodesis of the distal medial tibial physis. J Pediatr Orthop B. 2005. 14(6):436–438.
Article17. Beals RK. The treatment of ankle valgus by surface epiphysiodesis. Clin Orthop Relat Res. 1991. (266):162–169.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Effects of Partial Defect of Fibular Shaft on the Ankle in Children
- Nonunion in Bilateral Ball and Socket Ankle Joint
- Congenital Distal Tibio-fibular Synostosis: Case Report
- A Fibular Lengthening Osteotomy Combined with Calcaneal Osteotomy for Post-Traumatic Valgus Ankle Arthritis: A Case Report
- Treatment of Tibial Defect by Fibular Transposition using Ilizarov
