Prognostic Value of Modified Lateral Pillar Classification in Legg-Calve-Perthes Disease
- Affiliations
-
- 1Department of Orthopedic Surgery, Chonnam National University Medical School & Hospital, Gwangju, Korea. stjung@chonnam.ac.kr
- KMID: 999405
- DOI: http://doi.org/10.4055/cios.2009.1.4.222
Abstract
- BACKGROUND
To evaluate the usefulness of the modified lateral pillar classification as a prognostic factor in Legg-Calve-Perthes disease (LCPD).
METHODS
Thirty nine patients diagnosed with lateral pillar C in LCPD from May, 1977, to October, 2001 were reviewed, and their skeletal maturity was followed. The mean follow up duration was 12 years and 7 months (4 years, 6 months to 24 years, 9 months). Lateral pillar C classification was divided into C1 (50-75% collapse of the lateral pillar) and C2 (> 75%). All radiological and clinical prognostic factors were evaluated. The final results were evaluated according to the Stulberg classification.
RESULTS
Twenty one and 18 of the affected hips were in groups C1 and C2, respectively. According to the Stulberg classification, the final results of group C1 were better than those of C2 (p = 0.002). Patients with more head-at-risk signs had significantly poorer outcomes.
CONCLUSIONS
The modified lateral pillar classification has significant value for predicting the prognosis of LCPD.
MeSH Terms
Figure
-

Fig. 1 Schematic view of the modified lateral pillar C classification of Legg-Calvé-Perthes disease.
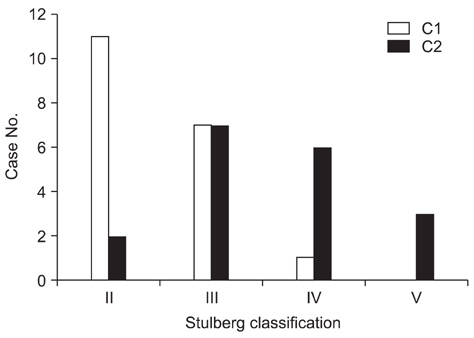
Fig. 2 Relation of the modified lateral pillar C classification with the Stulberg classification (chi-square test, p = 0.002).

Fig. 3 (A) An example of a left hip in group C1 of the modified lateral pillar classification in a patient who was 5.5 years old at presentation. This radiograph shows three radiographical head-at-risk signs, lateral subluxation of femoral head, calcification lateral to epiphysis and diffuse metaphyseal reaction. (B) Anteroposterior and frog-leg lateral radiograph of the pelvis made at the age of eighteen years showing a Stulberg II femoral head with slight differences between the two hips. The patient was treated with a brace.

Fig. 4 (A) An example of a right hip in group C1 of the modified lateral pillar classification in a patient who was 4.3 years old at presentation. The radiograph shows the four radiographical head-at-risk signs, lateral subluxation of femoral head, Gage's sign, calcification lateral to epiphysis and diffuse metaphyseal reaction. (B) Anteroposterior and frog-leg lateral radiograph of the pelvis, made at the age of sixteen years, showing the Stulberg III femoral head with marked differences between the two hips. The patient was treated with skin traction followed by a cast and with brace one year later.

Fig. 5 (A) An example of a left hip in group C2 of the modified lateral pillar classification in a patient who was 5.6 years old at presentation. This radiograph shows the two radiographical head-at-risk signs, Gage's sign and a diffuse metaphyseal reaction. (B) Anteroposterior and frog-leg lateral radiograph of the pelvis, made at the age of seventeen years, showing the Stulberg II femoral head with a decreased neck-shaft angle. The patient was treated with a brace.

Fig. 6 (A) An example of a right hip in group C2 of the modified lateral pillar classification in a patient who was 3.2 years old at presentation. This radiograph shows three significant radiographical head-at-risk signs, lateral subluxation of the femoral head, calcification lateral to the epiphysis, Gage's sign and a diffuse metaphyseal reaction. Among them, only three signs were related to the prognosis. (B) Anteroposterior and frog-leg lateral radiograph of the pelvis, made at the age of fifteen years, showing the Stulberg IV femoral head with a marked difference between the two hips. Affected hip shows a flattening of the femoral head.
Reference
-
1. Catterall A. The natural history of Perthes' disease. J Bone Joint Surg Br. 1971. 53(1):37–53.
Article2. Herring JA, Neustadt JB, Williams JJ, Early JS, Browne RH. The lateral pillar classification of Legg-Calvé-Perthes disease. J Pediatr Orthop. 1992. 12(2):143–150.3. McAndrew MP, Weinstein SL. A long-term follow-up of Legg-Calvé-Perthes disease. J Bone Joint Surg Am. 1984. 66(6):860–869.
Article4. Stulberg SD, Cooperman DR, Wallensten R. The natural history of Legg-Calvé-Perthes disease. J Bone Joint Surg Am. 1981. 63(7):1095–1108.
Article5. Yrjonen T, Poussa M, Hoikka V, Osterman K. Poor prognosis in atypical Perthes' disease: radiographic analysis of 19 hips after 35 years. Acta Orthop Scand. 1992. 63(4):399–402.6. Herring JA, Kim HT, Browne R. Legg-Calvé-Perthes disease. Part II: Prospective multicenter study of the effect of treatment on outcome. J Bone Joint Surg Am. 2004. 86(10):2121–2134.7. Wiig O, Terjesen T, Svenningsen S. Inter-observer reliability of the Stulberg classification in the assessment of Perthes disease. J Child Orthop. 2007. 1(2):101–105.
Article8. Herring JA, Kim HT, Browne R. Legg-Calvé-Perthes disease. Part I: Classification of radiographs with use of the modified lateral pillar and Stulberg classifications. J Bone Joint Surg Am. 2004. 86(10):2103–2120.9. Kamegaya M, Saisu T, Ochiai N, Hisamitsu J, Moriya H. A paired study of Perthes' disease comparing conservative and surgical treatment. J Bone Joint Surg Br. 2004. 86(8):1176–1181.
Article10. Hefti F, Clarke NM. The management of Legg-Calvé-Perthes' disease: is there a consensus? A study of clinical practice preferred by the members of the European Paediatric Orthopaedic Society. J Child Orthop. 2007. 1(1):19–25.11. Salter RB, Thompson GH. Legg-Calvé-Perthes disease: the prognostic significance of the subchondral fracture and a two-group classification of the femoral head involvement. J Bone Joint Surg Am. 1984. 66(4):479–489.
Article12. Ritterbusch JF, Shantharam SS, Gelinas C. Comparison of lateral pillar classification and Catterall classification of Legg-Calvé-Perthes' disease. J Pediatr Orthop. 1993. 13(2):200–202.13. Nathan Sambandam S, Gul A, Shankar R, Goni V. Reliability of radiological classifications used in Legg-Calvé-Perthes disease. J Pediatr Orthop B. 2006. 15(4):267–270.
Article14. Gent E, Antapur P, Mehta RL, Sudheer VM, Clarke NM. Predicting the outcome of Legg-Calve-Perthes' disease in children under 6 years old. J Child Orthop. 2007. 1(1):27–32.
Article15. Aksoy MC, Cankus MC, Alanay A, Yazici M, Caglar O, Alpaslan AM. Radiological outcome of proximal femoral varus osteotomy for the treatment of lateral pillar group-C Legg-Calvé-Perthes disease. J Pediatr Orthop B. 2005. 14(2):88–91.
Article16. Gigante C, Frizziero P, Turra S. Prognostic value of Catterall and Herring classification in Legg-Calvé-Perthes disease: follow-up to skeletal maturity of 32 patients. J Pediatr Orthop. 2002. 22(3):345–349.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Clinical Observation of the Legg-Calve-Perthes Disease: Preliminary Report
- Legg - Calve Perthes disease in Monozygotic Male Twins
- Osteochondritis Dissecans of Femoral Head Following Legg-Calve-Perthes Disease
- Innominate Osteotomy in Legg-Calve-Perthes Disease
- What Is the Usefulness of the Fragmentation Pattern of the Femoral Head in Managing Legg-Calve-Perthes Disease?
