Diffuse Infiltrative Lesion of the Breast: Clinical and Radiologic Features
- Affiliations
-
- 1Department of Radiology, Seoul St. Mary's Hospital, Seoul 137-701, Korea. rad-ksh@catholic.ac.kr
- 2Department of Radiology, Ewha Womans University Mokdong Hospital, Seoul 158-701, Korea.
- 3Department of Radiology, St. Paul's Hospital, Seoul 130-709, Korea.
- 4Department of Radiology, Incheon St. Mary's Hospital, Incheon 403-720, Korea.
- 5Department of Radiology, Bucheon St. Mary's Hospital, Bucheon 420-717, Korea.
- 6Department of Radiology, Uijongbu St. Mary's Hospital, Uijongbu 480-130, Korea.
- KMID: 991689
- DOI: http://doi.org/10.3348/kjr.2011.12.1.113
Abstract
- The purpose of this paper is to show the clinical and radiologic features of a variety of diffuse, infiltrative breast lesions, as well to review the relevant literature. Radiologists must be familiar with the various conditions that can diffusely involve the breast, including normal physiologic changes, benign disease and malignant neoplasm.
MeSH Terms
Figure
-
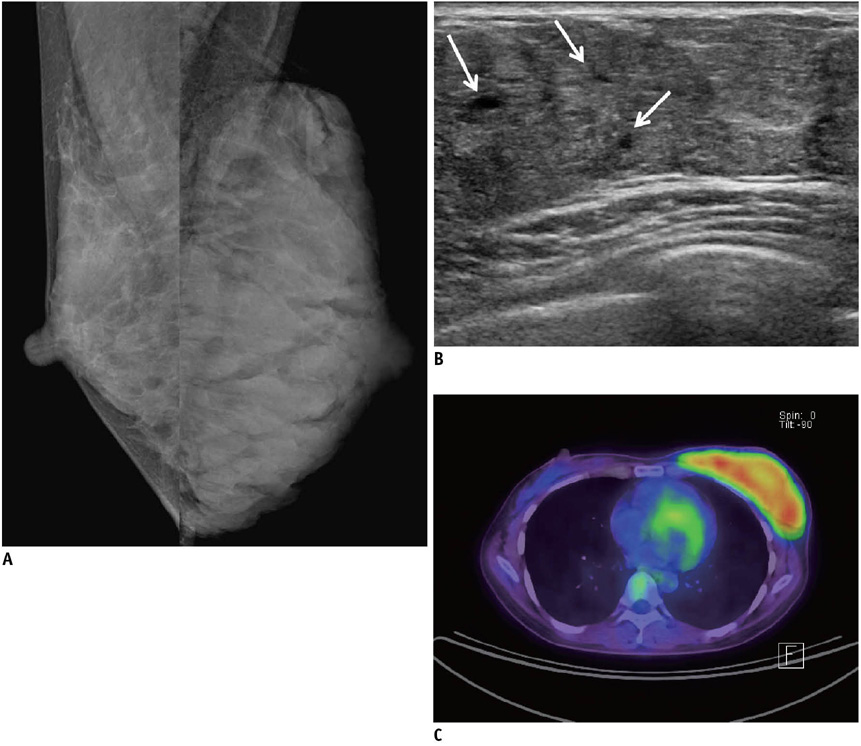
Fig. 1 Lactating breast in 31-year-old woman with past history of thyroidectomy due to thyroid cancer. Patient was nursing her infant with only her left breast. A. Mammogram shows asymmetrical enlargement of left breast with diffuse increase in density. B. Ultrasonogram of left breast reveals diffuse enlargement of glandular component with duct ectasia (arrows). C. FDG PET scanning shows diffuse and intense uptake in left breast (SUVmax = 4.7).
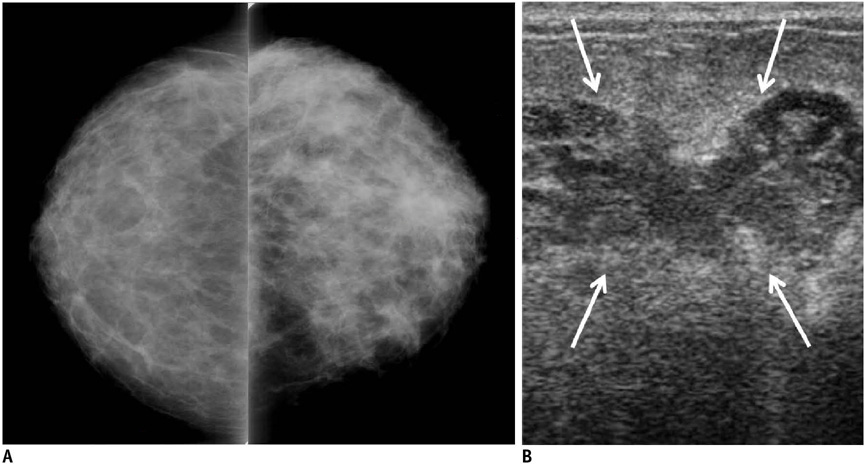
Fig. 2 Puerperal mastitis with abscess secondary to Staphylococcus hominis infection in 28-year-old lactating woman. A. Mammogram shows diffuse increase in density and trabecular thickening of left breast. B. Ultrasonogram show irregular, hypoechoic fluid collections that suggest abscess (arrows). Note edematous change of overlying skin and subcutaneous fat.
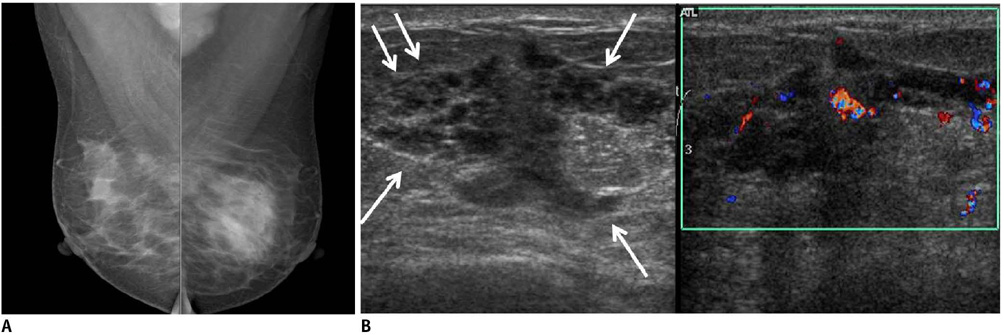
Fig. 3 Granulomatous mastitis in 31-year-old woman who was currently breast feeding at two years' postpartum. A. Mammogram shows asymmetric increased density in left breast. B. Ultrasonogram shows ill-defined, irregular tubular, heterogeneous hypoechoic lesion involving left breast (arrows). Note vascularity immediately adjacent to lesion on Doppler sonography.

Fig. 4 Pseudoangiomatous stromal hyperplasia in 47-year-old woman. A. Ultrasonogram demonstrates heterogeneously hypoechoic lesion with scattered cystic spaces (arrows) involving entire left breast. B. MRI of breast shows scattered cystic spaces of high signal intensity (black arrow) between diffuse and nodular low signals (white double arrows) on fat-saturated HASTE T2 image (TR/TE = 1100/118, flip angle: 150°). C. Fibrous tissue with low signal intensity on T2 image (white double arrows in B) shows homogeneous enhancement on contrast-enhanced T1 weighted image with fat suppression. (Material in Fig. 4 is quoted from Ryu et al.'s case report, which was published in Korean J Radiology in 2010).

Fig. 5 Left breast edema associated with left lung cancer in 89-year-old woman. Mammogram shows diffusely increased density with skin thickening and trabecular thickening of left breast.
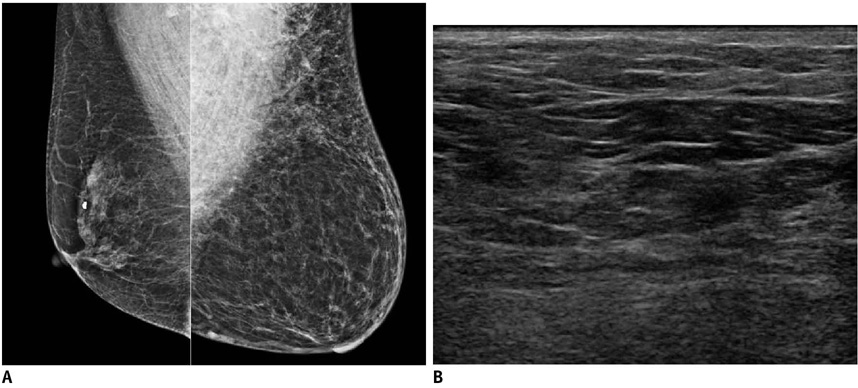
Fig. 6 Hemangioma of left breast with long-standing reddish purple skin change in 70-year-old woman. A. Mammogram shows diffusely increased density and trabecular thickening with enlargement of left breast. B. Ultrasonogram shows diffusely increased echogenicity of overlying subcutaneous fat layer of left breast.
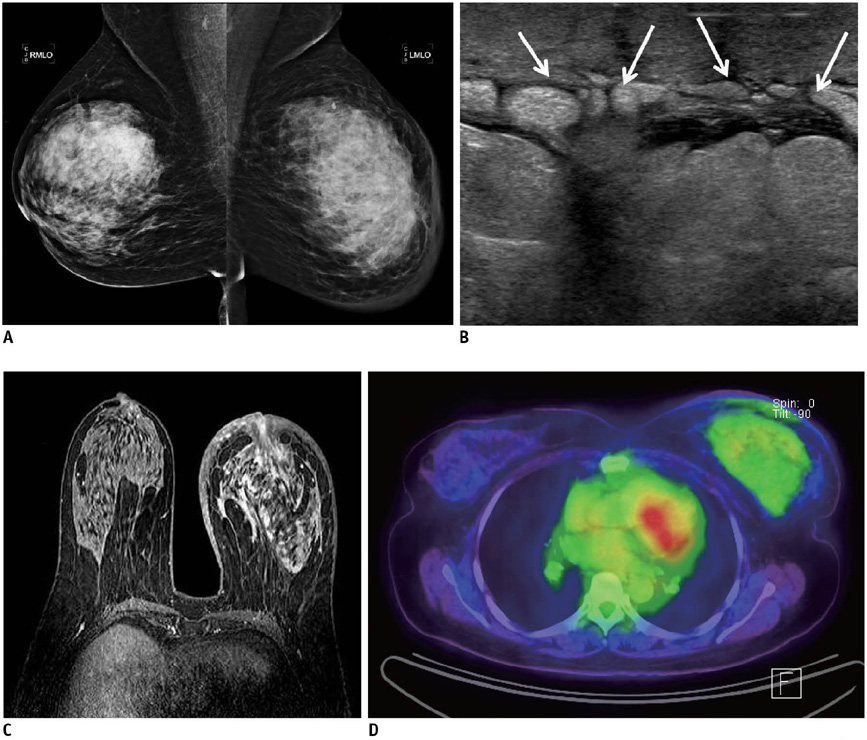
Fig. 7 Inflammatory breast cancer in 52-year-old woman. A. Mammogram shows diffusely increased density, trabecular thickening and skin thickening of left breast. B. Ultrasonogram of left breast shows marked skin thickening, subcutaneous edema and dilated lymphatic channels (arrows), which are all typical of breast edema pattern. C. Axial contrast-enhanced T1 weighted image shows diffuse, infiltrative, non-mass enhancement involving entire left breast (TR/TE = 5.1/2.5). D. FDG PET scanning shows diffuse uptake of right breast with focal uptake on overlying thicken skin (SUVmax = 2.3).
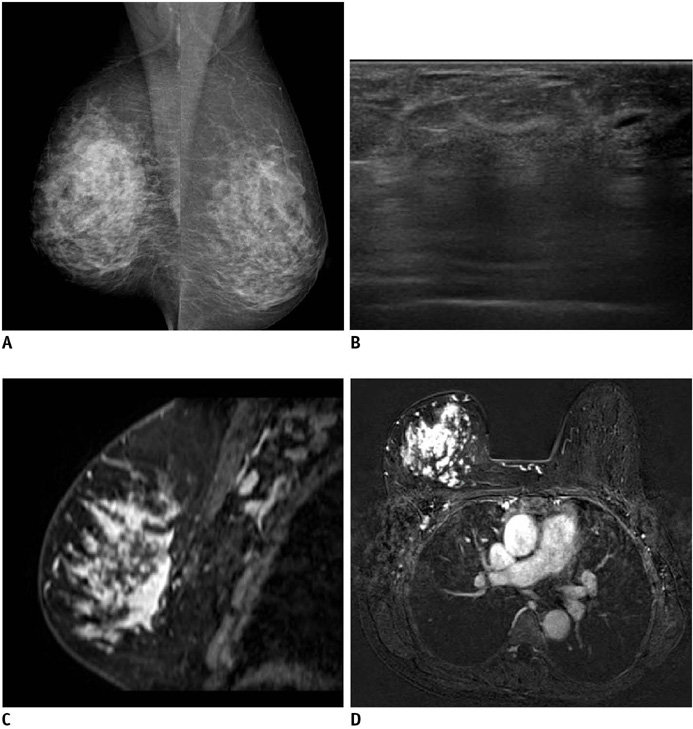
Fig. 8 Invasive lobular carcinoma in 50-year-old woman who presented with hardness and decrease in size of right breast. A. Mammogram shows diffuse skin thickening and trabecular thickening of right breast. B. Ultrasonogram of right breast shows diffuse posterior acoustic shadowing without discrete mass. C, D. Sagittal (C) and axial (D) contrast-enhanced T1 weighted images, respectively, reveal non-mass enhancement involving nearly entire right breast (TR/TE = 4.2/2.0).
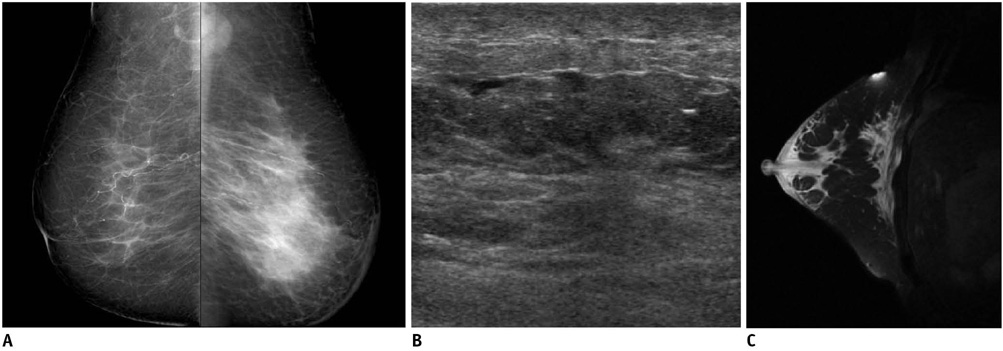
Fig. 9 Secondary lymphoma to breast in 78-year-old woman with left breast enlargement. A. Mammogram shows diffuse increased opacity throughout entire left breast with skin thickening. Note enlarged lymph nodes in left axilla on left mediolateral oblique mammogram. B. Ultrasonogram shows diffuse skin and subcutaneous edema of left breast. C. Sagittal T2 weighted image shows diffuse breast edema of high signal intensity in left breast (TR/TE = 4000/81.9).

Fig. 10 Metastatic rhabdomyosarcoma to breasts in 30-year-old woman with bilateral enlargement of breasts. She had history of sinonasal rhabdomyosarcoma that was treated by chemotherapy and radiation therapy 21 months previously. A. Chest CT scan shows dense parenchyma with subtle nodular infiltration in both breasts. B. Ultrasonogram shows heterogeneous, infiltrative hypoechoic lesion that occupies majority of breast parenchyma.
Reference
-
1. Hogge JP, De Paredes ES, Magnant CM, Lage J. Imaging and management of breast masses during pregnancy and lactation. Breast J. 1999. 5:272–283.2. Hicks RJ, Binns D, Stabin MG. Pattern of uptake and excretion of (18) F-FDG in the lactating breast. J Nucl Med. 2001. 42:1238–1242.3. Yasuda S, Fujii H, Takahashi W, Takagi S, Ide M, Shohtsu A. Lactating breast exhibiting high F-18 FDG uptake. Clin Nucl Med. 1998. 23:767–768.4. Crowe DJ, Helvie MA, Wilson TE. Breast infection. Mammographic and sonographic findings with clinical correlation. Invest Radiol. 1995. 30:582–587.5. Ulitzsch D, Nyman MK, Carlson RA. Breast abscess in lactating women: US-guided treatment. Radiology. 2004. 232:904–909.6. Han BK, Choe YH, Park JM, Moon WK, Ko YH, Yang JH, et al. Granulomatous mastitis: mammographic and sonographic appearances. AJR Am J Roentgenol. 1999. 173:317–320.7. Fletcher A, Magrath IM, Riddell RH, Talbot IC. Granulomatous mastitis: a report of seven cases. J Clin Pathol. 1982. 35:941–945.8. Going JJ, Anderson TJ, Wilkinson S, Chetty U. Granulomatous lobular mastitis. J Clin Pathol. 1987. 40:535–540.9. Lee JH, Oh KK, Kim EK, Kwack KS, Jung WH, Lee HK. Radiologic and clinical features of idiopathic granulomatous lobular mastitis mimicking advanced breast cancer. Yonsei Med J. 2006. 47:78–84.10. Van Ongeval C, Schraepen T, Van Steen A, Baert AL, Moerman P. Idiopathic granulomatous mastitis. Eur Radiol. 1997. 7:1010–1012.11. Ibrahim RE, Sciotto CG, Weidner N. Pseudoangiomatous hyperplasia of mammary stroma. Some observations regarding its clinicopathologic spectrum. Cancer. 1989. 63:1154–1160.12. Ryu EM, Whang IY, Chang ED. Rapidly growing bilateral pseudoangiomatous stromal hyperplasia of the breast. Korean J Radiol. 2010. 11:355–358.13. Teh HS, Chiang SH, Leung JW, Tan SM, Mancer JF. Rapidly enlarging tumoral pseudoangiomatous stromal hyperplasia in a 15-year-old patient: distinguishing sonographic and magnetic resonance imaging findings and correlation with histologic findings. J Ultrasound Med. 2007. 26:1101–1106.14. Kwak JY, Kim EK, Chung SY, You JK, Oh KK, Lee YH, et al. Unilateral breast edema: spectrum of etiologies and imaging appearances. Yonsei Med J. 2005. 46:1–7.15. Toh CK, Leong SS, Thng CH, Tan EH. Unilateral breast edema in two patients with malignant pleural effusion. Tumori. 2004. 90:501–503.16. Rosen PP. Vascular tumors of the breast. V. Nonparenchymal hemangiomas of mammary subcutaneous tissues. Am J Surg Pathol. 1985. 9:723–729.17. Rosen PP. Vascular tumors of the breast. III. Angiomatosis. Am J Surg Pathol. 1985. 9:652–658.18. Siewert B, Jacobs T, Baum JK. Sonographic evaluation of subcutaneous hemangioma of the breast. AJR Am J Roentgenol. 2002. 178:1025–1027.19. Mesurolle B, Sygal V, Lalonde L, Lisbona A, Dufresne MP, Gagnon JH, et al. Sonographic and mammographic appearances of breast hemangioma. AJR Am J Roentgenol. 2008. 191:W17–W22.20. Dershaw DD, Moore MP, Liberman L, Deutch BM. Inflammatory breast carcinoma: mammographic findings. Radiology. 1994. 190:831–834.21. Ellis DL, Teitelbaum SL. Inflammatory carcinoma of the breast. A pathologic definition. Cancer. 1974. 33:1045–1047.22. Baslaim MM, Bakheet SM, Bakheet R, Ezzat A, El-Foudeh M, Tulbah A. 18-Fluorodeoxyglucose-positron emission tomography in inflammatory breast cancer. World J Surg. 2003. 27:1099–1104.23. Dixon JM, Anderson TJ, Page DL, Lee D, Duffy SW. Infiltrating lobular carcinoma of the breast. Histopathology. 1982. 6:149–161.24. Krecke KN, Gisvold JJ. Invasive lobular carcinoma of the breast: mammographic findings and extent of disease at diagnosis in 184 patients. AJR Am J Roentgenol. 1993. 161:957–960.25. Butler RS, Venta LA, Wiley EL, Ellis RL, Dempsey PJ, Rubin E. Sonographic evaluation of infiltrating lobular carcinoma. AJR Am J Roentgenol. 1999. 172:325–330.26. Vizcaíno I, Torregrosa A, Higueras V, Morote V, Cremades A, Torres V, et al. Metastasis to the breast from extramammary malignancies: a report of four cases and a review of literature. Eur Radiol. 2001. 11:1659–1665.27. Chung SY, Oh KK. Imaging findings of metastatic disease to the breast. Yonsei Med J. 2001. 42:497–502.28. Lee SH, Park JM, Kook SH, Han BK, Moon WK. Metastatic tumors to the breast: mammographic and ultrasonographic findings. J Ultrasound Med. 2000. 19:257–262.29. Arora R, Robinson WA. Breast metastases from malignant melanoma. J Surg Oncol. 1992. 50:27–29.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Primary Systemic Amyloidosis Presenting as Swollen Dense Breast: A Case Report
- Infiltrative invasion of the diaphragm: an uncommon manifestation of recurrent hepatocellular carcinoma
- DILD (diffuse infiltrative lung disease); Radiologic Diagnostic Approach According to High-Resolution CT Pattern
- Ultrasonographic Findings of Apocrine Lesions Arising from the Breast
- Ultrasonographic and Mammographic Findings of Gynecomastia
