Yonsei Med J.
2008 Jun;49(3):503-506. 10.3349/ymj.2008.49.3.503.
A Case of Multiple Endocrine Neoplasia Type 1 Combined with Papillary Thyroid Carcinoma
- Affiliations
-
- 1Department of Endocrinology and Metabolism, Internal Medicine, Yonsei University College of Medicine, Seoul, Korea. acw@yuhs.ac
- KMID: 724269
- DOI: http://doi.org/10.3349/ymj.2008.49.3.503
Abstract
- This is the first report of papillary thyroid carcinoma combined with multiple endocrine neoplasia type 1 (MEN1) in Korea. MEN1 is a hereditary disease comprising neoplastic disorders such as pituitary, parathyroid and pancreatic neuroendocrine tumor, such as gastrinoma. But papillary thyroid cancer was never regarded as its component before in Korea. Herein we present a 39-year-old woman who manifested typical features of MEN1 with a coincidental papillary thyroid carcinoma. Although the family history of MEN1 was definite, her genetic analysis of DNA had revealed no germline mutation in MEN1 gene locus. Unidentified culprit gene unable us further genetic study to find LOH (loss of heterogeneity) in 11q13, the possible explanation of papillary thyroid carcinoma as a new component of MEN1. As we have first experienced a case of MEN1 combined with papillary thyroid carcinoma in Korea, we report it with the review of literature.
Keyword
MeSH Terms
Figure
-

Fig. 1 Thyroid US shows about 1.5 cm irregular mass at upper pole of right thyroid gland.

Fig. 2 Sellar MRI shows 0.9 × 0.6 mm sized microadenoma in left portion of pituitary gland.
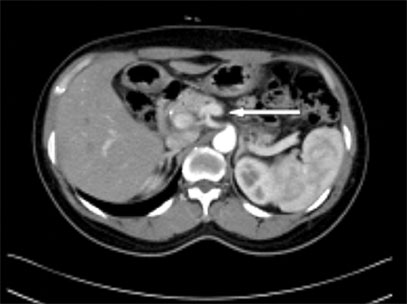
Fig. 3 Abdominal dynamic CT shows 0.68 cm sized arterial enhancing mass at pancreatic body.

Fig. 4 Histologic feature of parathyroid hyperplasia (H&E stain, × 100).

Fig. 5 Histologic feature of thyroid papillary carcinoma showing inclusion body (H&E stain, × 100).
Reference
-
1. Lairmore TC, Piersall LD, DeBenedetti MK, Dilley WG, Mutch MG, Whelan AJ, et al. Clinical genetic testing and early surgical intervention in patients with multiple endocrine neoplasia type1 (MEN1). Ann Surg. 2004. 239:637–645. discussion 645-7.2. Chandrasekharappa SC, Guru SC, Manickam P, Olufemi SE, Collins FS, Emmert-Buck MR, et al. Positional cloning of the gene for multiple endocrine neoplasia type1. Science. 1997. 276:404–407.3. Dong Q, Debelenko LV, Chandrasekharappa SC, Emmert-Buck MR, Zhuang Z, Guru SC, et al. Loss of heterozygosity at 11q13: analysis of pituitary tumors, lung carcinoids, lipomas, and other uncommon tumors in subjects with familial multiple endocrine neoplasia type1. J Clin Endocrinol Metab. 1997. 82:1416–1420.
Article4. Desai D, McPherson LA, Higgins JP, Weigel RJ. Genetic analysis of a papillary thyroid carcinoma in a patient with MEN1. Ann Surg Oncol. 2001. 8:342–346.5. Vortmeyer AO, Lubensky IA, Skarulis M, Li G, Moon YW, Park WS, et al. Multiple endocrine neoplasia type 1: atypical presentation, clinical course, and genetic analysis of multiple tumors. Mod Pathol. 1999. 12:919–924.6. Park JH, Kim IJ, Kang HC, Lee SH, Shin Y, Kim KH, et al. Germline mutations of the MEN1 gene in Korean families with multiple endocrine neoplasia type 1 (MEN1) or MEN1-related disorders. Clin Genet. 2003. 64:48–53.
Article7. Larsson C, Skogseid B, Oberg K, Nakamura Y, Nordenskjöld M. Multiple endocrine neoplasia type1 gene maps to chromosome 11 and is lost in insulinoma. Nature. 1988. 332:85–87.
Article8. Friedman E, Sakaguchi K, Bale AE, Falchetti A, Streeten E, Zimering MB, et al. Clonality of parathyroid tumors in familial multiple endocrine neoplasia type1. N Engl J Med. 1989. 321:213–218.
Article9. Chandrasekharappa SC, Teh BT. Functional studies of the MEN1 gene. J Intern Med. 2003. 253:606–615.
Article10. Nishiyama RH, Farhi D, Thompson NW. Radiation exposure and the simultaneous occurrence of primary hyperparathyroidism and thyroid nodules. Surg Clin North Am. 1979. 59:65–75.11. Prinz RA, Barbato AL, Braithwaite SS, Brooks MH, Emanuele MA, Gordon DL, et al. Simultaneous primary hyperparathyroidism and nodular thyroid disease. Surgery. 1982. 92:454–458.12. Attie JN, Vardhan R. Association of hyperparathyroidism with nonmedullary thyroid carcinoma: review of 31 cases. Head Neck. 1993. 15:20–23.13. Hedman I, Tisell LE. Associated hyperparathyroidism and nonmedullary thyroid carcinoma: the etiologic role of radiation. Surgery. 1984. 95:392–397.14. Smith MA, McHenry C, Oslapas R, Hofmann C, Hessel P, Paloyan E. Altered TSH levels associated with increased serum 1,25-dihydroxyvitamin D3: a possible link between thyroid and parathyroid disease. Surgery. 1989. 106:987–991.15. Arem R, Lim-Abrahan MA, Mallette LE. Concomitant Graves' disease and primary hyperparathyroidism. Influence of hyperthyroidism on serum calcium and parathyroid hormone. Am J Med. 1986. 80:693–698.
Article16. Regal M, Páramo C, Luna Cano R, Pérez Méndez LF, Sierra JM, Rodríguez I, et al. Coexistence of primary hyperparathyroidism and thyroid disease. J Endocrinol Invest. 1999. 22:191–197.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Multiple Endocrine Neoplasia and Familial Medullary Thyroid Carcinoma
- A Case of Multiple Endocrine Neoplasia type 3 With Multiple Mucosal Neuroma
- A Case of Multiple Endocrine Neoplasia Type 1 with Papillary Thyroid Carcinoma
- A Case of Papillary Thyroid Carcinoma Combined with Multiple Endocrine Neoplasia Type 2A
- A Case of Familial Medullary Thyroid Carcinoma
