Ulcerative colitis-associated neoplasms often harbor poor prognostic histologic components with low detection by biopsy
- Sakakibara R
 1
1 - Sugimoto S1
- Takabayashi K2
- Kiyohara H1
- Wakisaka Y1
- Kaieda Y1
- Kawaida M3
- Yoshimatsu Y1
- Sujino T2
- Hosoe N4
- Kato M2
- Shimoda M3
- Mikami Y1
- Iwao Y4
- Kanai T1
- Affiliations
-
- 1Division of Gastroenterology and Hepatology, Department of Internal Medicine, Keio University School of Medicine, Tokyo, Japan
- 2Center for Diagnostic and Therapeutic Endoscopy, Keio University School of Medicine, Tokyo, Japan
- 3Department of Pathology, Keio University School of Medicine, Tokyo, Japan
- 4Center for Preventive Medicine, Keio University School of Medicine, Tokyo, Japan
- KMID: 2560293
- DOI: http://doi.org/10.5217/ir.2024.00006
Abstract
- Background/Aims
Poorly differentiated adenocarcinoma, signet-ring cell carcinoma, and mucinous adenocarcinoma (por/sig/muc), which are considered to be histologic subtypes with a poor prognosis, occur more frequently with colitis-associated cancer than with sporadic tumors. However, their invasiveness and manifestations are unclear. This study aimed to determine the prevalence of the por/sig/muc component in ulcerative colitis-associated neoplasms (UCANs) and its association with invasiveness and to clarify its clinicohistologic and endoscopic features.
Methods
This retrospective observational study included patients diagnosed with ulcerative colitis-associated high-grade dysplasia or adenocarcinoma from 1997 to 2022 who were divided according to the presence or absence of a por/sig/muc component.
Results
Thirty-five patients had UCAN with a por/sig/muc component and 66 had UCAN without this component. The 5-year survival rate was significantly lower in the por/sig/muc group than in the tub group (67% vs. 96%, P= 0.001), which was attributed to disease above stage III and depth to below the subserosa. Biopsy-based diagnosis before resection detected a por/sig/muc component in only 40% of lesions (14/35). Lesions with a por/sig/muc component were prevalent even in the early stages: stage 0 (4/36, 11%), I (8/20, 40%), II (7/12, 58%), III (10/14, 71%), and IV (6/8, 75%).
Conclusions
This is the first investigation that shows UCANs with a por/sig/muc component tended to be deeply invasive and were often not recognized preoperatively. Endoscopists should be aware that UCAN often has a por/sig/muc component that is not always recognized on biopsy, and the optimal treatment strategy needs to be carefully considered.
Figure
-
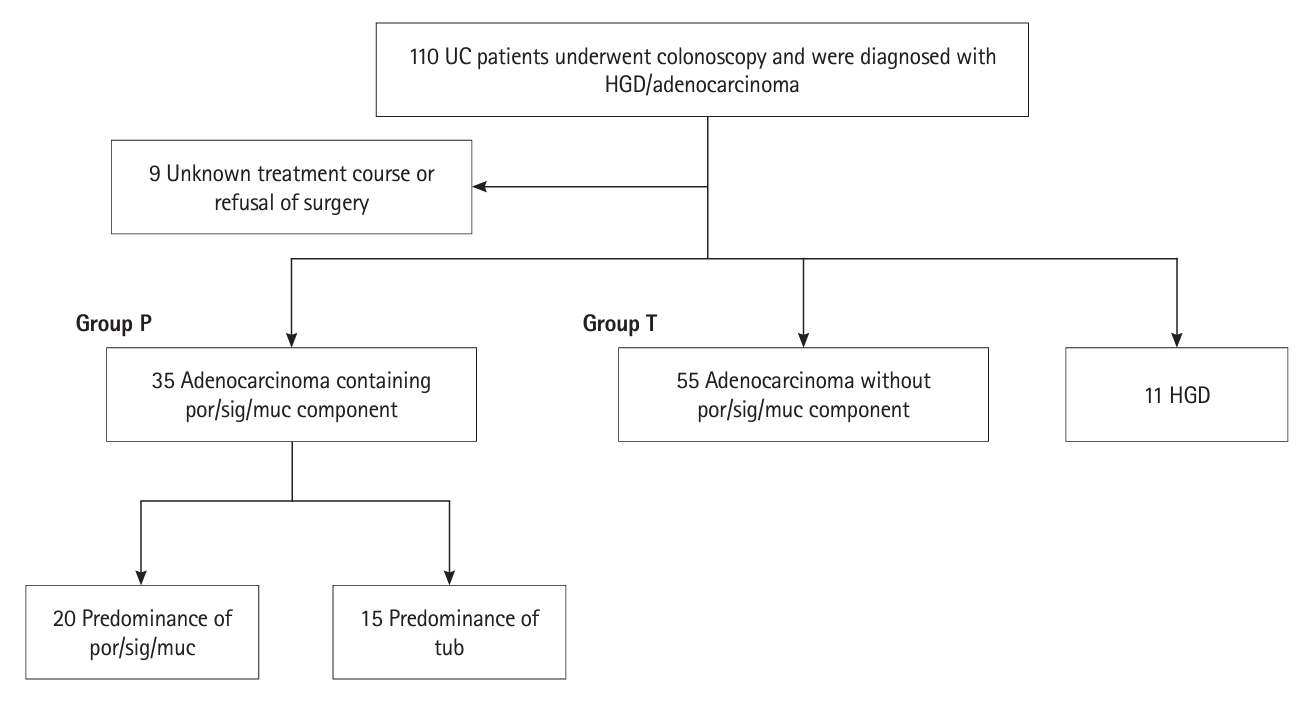
Fig. 1. Flow of patients through the study. One hundred and one of 110 patients with ulcerative colitis (UC) and HGD/adenocarcinoma were enrolled and divided into a group with por/sig/muc components (n=35; Group P) and a group without por/sig/muc components (n=55; Group T) and HGD (n=11). The Group P was subdivided according to whether it contained more por/sig/muc components (n=20) or more tub components (n=15). HGD, high-grade dysplasia; por, poorly differentiated adenocarcinoma; sig, signet-ring cell carcinoma; muc, mucinous adenocarcinoma; tub, tubular adenocarcinoma.
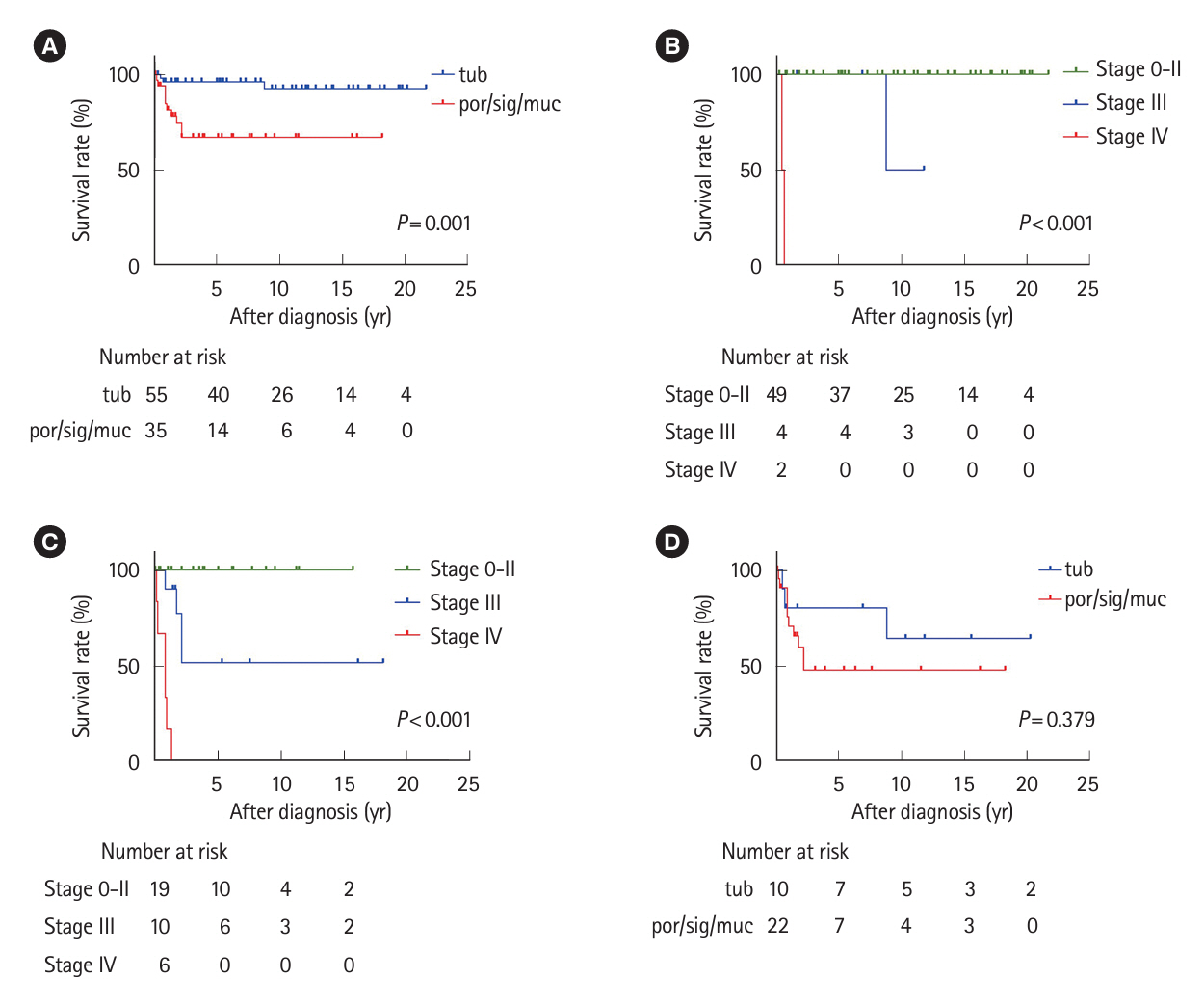
Fig. 2. Kaplan-Meier survival curves for patients after diagnosis of ulcerative colitis-associated neoplasms. (A) Cumulative survival of all patients with adenocarcinoma in the por/sig/muc (Group P) and tub (Group T) groups. (B, C) Cumulative survival rates for patients in the Group T (B) and Group P (C) divided into stages 0–II, III, and IV. (D) Cumulative survival rates of patients with a tumor depth of at least subserosa divided into Group P and Group T. por, poorly differentiated adenocarcinoma; sig, signet-ring cell carcinoma; muc, mucinous adenocarcinoma; tub, tubular adenocarcinoma.
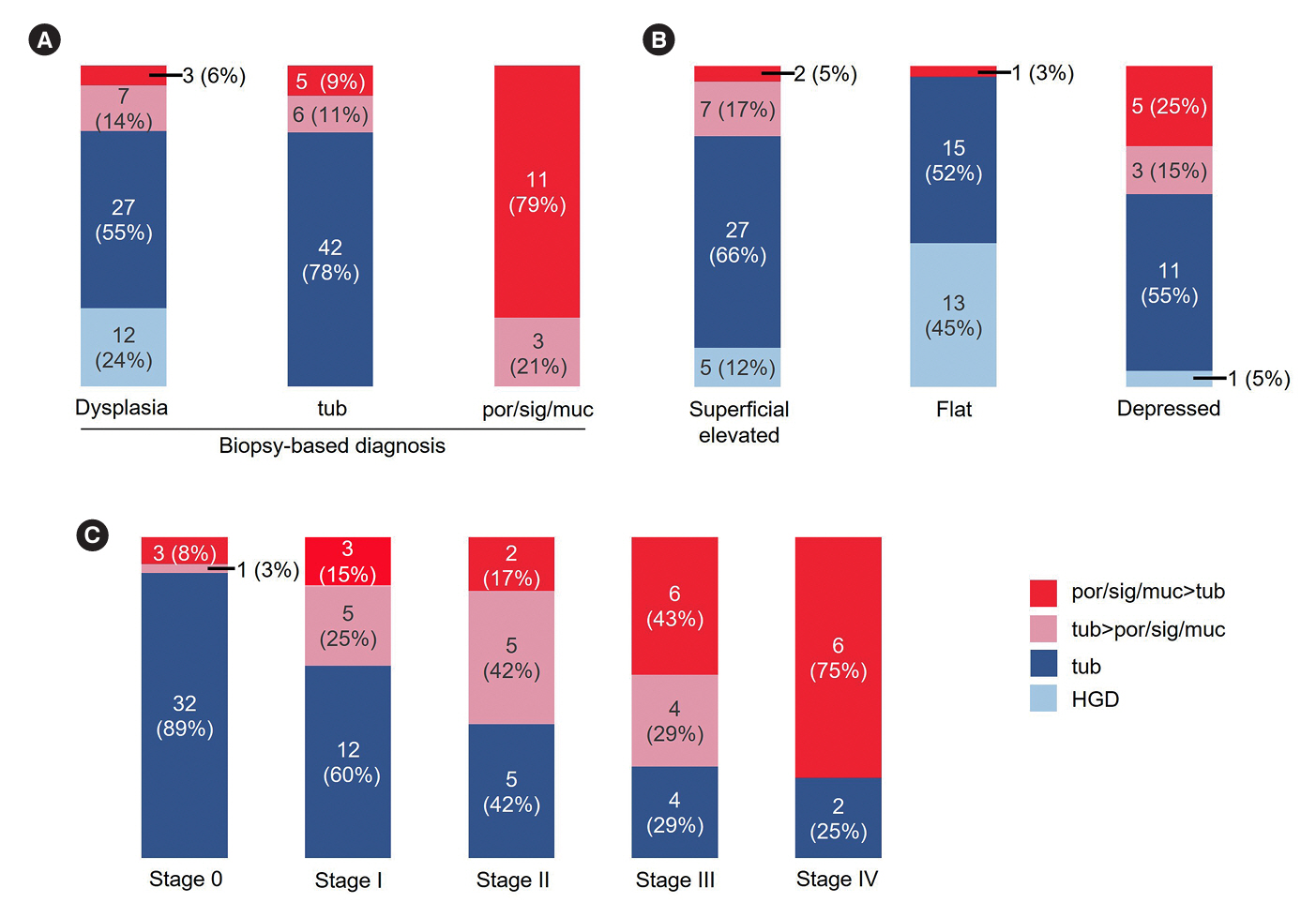
Fig. 3. Lesion histology according to targeted biopsy diagnosis, SCENIC classification, and staging. (A) Discrepancies in the final histologic diagnosis in each resected specimen diagnosed as dysplasia, tub, or por/sig/muc on biopsy. Only cases of identifiable lesions in which both targeted biopsy and resection pathology information were available were analyzed. (B) Proportion of lesions according to the SCENIC classification defined by colonoscopy with final histologic diagnosis. (C) Comparison of the proportions of histologic types of lesions at each disease stage. tub, tubular adenocarcinoma; por, poorly differentiated adenocarcinoma; sig, signet-ring cell carcinoma; muc, mucinous adenocarcinoma; HGD, high-grade dysplasia.
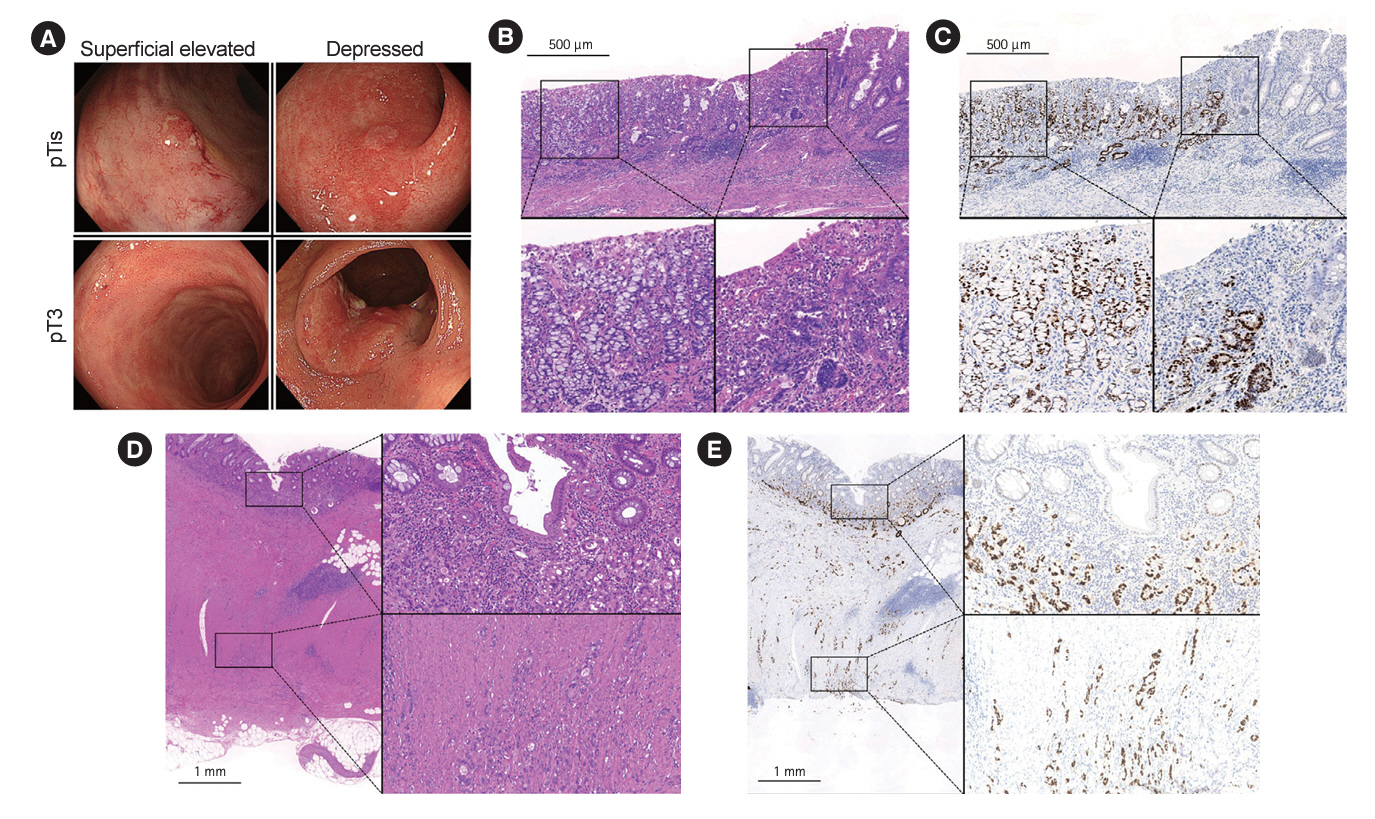
Fig. 4. Representative endoscopic and histologic findings in the Group P. (A) Images of CAC in the Group P, which are classified in the same SCENIC classification category but have markedly different tumor depths. Lesions with at least a portion depressed below the level of the mucosa were presented as depressed lesions. (B, C) Representative H&E staining (B) and p53 immunostaining (C) of CAC (right top panel, Fig. 4A) with sig (left bottom panel) and tub (right bottom panel) tumor histology differing by site because of intratumoral heterogeneity. (D, E) Representative H&E staining (D) and p53 immunostaining (E) of CAC (left bottom panel, Fig. 4A) which is difficult to detect from the surface but has a por component infiltrating to the subserosa. Inset shows higher magnification. CAC, colitis-associated neoplasia; Group P, por/sig/muc group; por, poorly differentiated adenocarcinoma; sig, signet-ring cell carcinoma; muc, mucinous adenocarcinoma; tub, tubular adenocarcinoma; H&E, hematoxylin and eosin.

Reference
-
1. Turner D, Ricciuto A, Lewis A, et al. STRIDE-II: an update on the Selecting Therapeutic Targets in Inflammatory Bowel Disease (STRIDE) Initiative of the International Organization for the Study of IBD (IOIBD): determining therapeutic goals for treat-to-target strategies in IBD. Gastroenterology. 2021; 160:1570–1583.
Article2. Eaden JA, Abrams KR, Mayberry JF. The risk of colorectal cancer in ulcerative colitis: a meta-analysis. Gut. 2001; 48:526–535.3. Olén O, Erichsen R, Sachs MC, et al. Colorectal cancer in ulcerative colitis: a Scandinavian population-based cohort study. Lancet. 2020; 395:123–131.
Article4. Tsai L, Ma C, Dulai PS, et al. Contemporary risk of surgery in patients with ulcerative colitis and Crohn’s disease: a meta-analysis of population-based cohorts. Clin Gastroenterol Hepatol. 2021; 19:2031–2045.
Article5. Shah SC, Itzkowitz SH. Colorectal cancer in inflammatory bowel disease: mechanisms and management. Gastroenterology. 2022; 162:715–730.
Article6. Mir-Madjlessi SH, Farmer RG, Easley KA, Beck GJ. Colorectal and extracolonic malignancy in ulcerative colitis. Cancer. 1986; 58:1569–1574.
Article7. Lu C, Schardey J, Zhang T, et al. Survival outcomes and clinicopathological features in inflammatory bowel disease-associated colorectal cancer: a systematic review and meta-analysis. Ann Surg. 2022; 276:e319–e330.8. Sugimoto S, Shimoda M, Iwao Y, et al. Intramucosal poorly differentiated and signet-ring cell components in patients with ulcerative colitis-associated high-grade dysplasia. Dig Endosc. 2019; 31:706–711.
Article9. Watanabe T, Konishi T, Kishimoto J, et al. Ulcerative colitis-associated colorectal cancer shows a poorer survival than sporadic colorectal cancer: a nationwide Japanese study. Inflamm Bowel Dis. 2011; 17:802–808.
Article10. Laine L, Kaltenbach T, Barkun A, et al. SCENIC international consensus statement on surveillance and management of dysplasia in inflammatory bowel disease. Gastroenterology. 2015; 148:639–651.
Article11. Murthy SK, Feuerstein JD, Nguyen GC, Velayos FS. AGA clinical practice update on endoscopic surveillance and management of colorectal dysplasia in inflammatory bowel diseases: expert review. Gastroenterology. 2021; 161:1043–1051.
Article12. Gordon H, Biancone L, Fiorino G, et al. ECCO guidelines on inflammatory bowel disease and malignancies. J Crohns Colitis. 2023; 17:827–854.13. Ueno H, Mochizuki H, Hashiguchi Y, et al. Risk factors for an adverse outcome in early invasive colorectal carcinoma. Gastroenterology. 2004; 127:385–394.
Article14. Wang AY, Hwang JH, Bhatt A, Draganov PV. AGA clinical practice update on surveillance after pathologically curative endoscopic submucosal dissection of early gastrointestinal neoplasia in the United States: commentary. Gastroenterology. 2021; 161:2030–2040.
Article15. Sugimoto S, Naganuma M, Iwao Y, et al. Endoscopic morphologic features of ulcerative colitis-associated dysplasia classified according to the SCENIC consensus statement. Gastrointest Endosc. 2017; 85:639–646.16. Mutaguchi M, Naganuma M, Sugimoto S, et al. Difference in the clinical characteristic and prognosis of colitis-associated cancer and sporadic neoplasia in ulcerative colitis patients. Dig Liver Dis. 2019; 51:1257–1264.
Article17. Sugimoto S, Iwao Y, Shimoda M, et al. Epithelium replacement contributes to field expansion of squamous epithelium and ulcerative colitis-associated neoplasia. Gastroenterology. 2022; 162:334–337.18. Takabayashi K, Sugimoto S, Nanki K, et al. Characteristics of flat-type ulcerative colitis-associated neoplasia on chromoendoscopic imaging with indigo carmine dye spraying. Dig Endosc. 2024; 36:446–454.
Article19. Schroeder KW, Tremaine WJ, Ilstrup DM. Coated oral 5-aminosalicylic acid therapy for mildly to moderately active ulcerative colitis: a randomized study. N Engl J Med. 1987; 317:1625–1629.
Article20. Kobayashi S, Fujimori T, Mitomi H, et al. Immunohistochemical assessment of a unique basal pattern of p53 expression in ulcerative-colitis-associated neoplasia using computer-assisted cytometry. Diagn Pathol. 2014; 9:99.
Article21. Matkowskyj KA, Chen ZE, Rao MS, Yang GY. Dysplastic lesions in inflammatory bowel disease: molecular pathogenesis to morphology. Arch Pathol Lab Med. 2013; 137:338–350.
Article22. Japanese Society for Cancer of the Colon and Rectum. Japanese classification of colorectal, appendiceal, and anal carcinoma: the 3rd English edition. Tokyo: Kanehara & Co., Ltd.;2019.23. Kang H, O’Connell JB, Maggard MA, Sack J, Ko CY. A 10-year outcomes evaluation of mucinous and signet-ring cell carcinoma of the colon and rectum. Dis Colon Rectum. 2005; 48:1161–1168.24. Choi CR, Al Bakir I, Ding NJ, et al. Cumulative burden of inflammation predicts colorectal neoplasia risk in ulcerative colitis: a large single-centre study. Gut. 2019; 68:414–422.
Article25. Choi CH, Ignjatovic-Wilson A, Askari A, et al. Low-grade dysplasia in ulcerative colitis: risk factors for developing high-grade dysplasia or colorectal cancer. Am J Gastroenterol. 2015; 110:1461–1471.
Article26. Bak MTJ, Albéniz E, East JE, et al. Endoscopic management of patients with high-risk colorectal colitis-associated neoplasia: a Delphi study. Gastrointest Endosc. 2023; 97:767–779.
Article27. Mikami T, Yoshida T, Numata Y, et al. Invasive behavior of ulcerative colitis-associated carcinoma is related to reduced expression of CD44 extracellular domain: comparison with sporadic colon carcinoma. Diagn Pathol. 2011; 6:30.
Article28. Kaltenbach T, Holmes I, Nguyen-Vu T, et al. Longitudinal outcomes of the endoscopic resection of nonpolypoid dysplastic lesions in patients with inflammatory bowel disease. Gastrointest Endosc. 2023; 97:934–940.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Malignant Lymphoma in Patient with Ulcerative Colitis
- Can histologic remission be a better prognostic factor and therapeutic target beyond endoscopic mucosal healing in patients with ulcerative colitis?
- Recent Advances in Understanding Colorectal Cancer and Dysplasia Related to Ulcerative Colitis
- Histopathological Features of Endoscopic Biopsies in Ischemic Colitis
- Trends in the incidence of ulcerative colitis in Korea
